Although the worldwide incidence of allergic rhinitis has been on the rise, many experts debate whether that trend is due to mounting air pollution, indoor environmental factors, improved hygiene practices, genetics, geographic location or all of the above.
Explore This Issue
March 2010There may not be one answer to the question of why allergic rhinitis is becoming more common, but there is little doubt that the disorder has been increasing at an alarming rate. According to the American College of Allergy, Asthma and Immunology (ACAAI), allergic rhinitis has increased 100 percent in each of the last three decades.
ENT Today recently spoke with experts on the subject to help unravel some of the mysteries surrounding the rise in allergic rhinitis.

Pollution
“There is clear evidence that much of that increase has occurred in developing countries,” said Matthew Ryan, MD, assistant professor of otolaryngology at the University of Texas Southwestern Medical Center in Dallas. Although it is difficult to get a handle on the epidemiology of allergic rhinitis, studies have shown that the occurrence of allergic rhinitis is increasing in areas that used to have a low prevalence, such as developing countries, Dr. Ryan said (Allergy. 2008;63 Suppl 86:8-160).
Although experts haven’t fully explained that trend, most speculate that it is related to the fact that those countries are adopting more western lifestyles. “More people are moving from rural, agricultural settings, which traditionally have had lower rates of allergies, to more urban settings, which have higher levels of air pollution,” Dr. Ryan said.
Three recent European studies support the hypothesis that an increase in air pollution has contributed to a rise in allergic rhinitis. The main culprits? Growing concentrations of sulfur dioxide (SO2), ozone (O3) and carbon monoxide (CO).
In the first study, researchers at the Royal Free and University College Medical School in London found that increased exposure to SO2 in children was associated with a 24.5 percent rise in office visits for allergic rhinitis, while increased exposure to ozone was associated with a 37.6 percent rise (Am J Epidemiol. 2001;153(7):704-714). The association with SO2 remained highly significant in the presence of other pollutants, according to the authors, “suggesting that air pollution worsens allergic rhinitis symptoms, leading to substantial increases in office visits.”
The second study, of 20,455 children seen at seven different care sites in Spain, found that annual average concentrations of SO2 were significantly associated with a higher prevalence of recent severe asthma, rhinitis and rhinoconjunctivitis (Arch Bronconeumol. 2009;45(5):224-229). Carbon monoxide was associated with a higher prevalence of rhinitis, rhinoconjunctivitis and eczema. The authors concluded that the data establish a clear link between the pollutants and the children’s worsening allergic disease.
In the third study, ozone exposure resulted in epithelial disruption and increased permeability, inflammatory cell influx and proliferative and secretory responses in the nasal epithelium (J Toxicol Environ Health B Crit Rev. 2003;6(5):521-568). The effects “…had a priming effect on the late-phase response to allergen challenge, providing new insights into the pathophysiology of respiratory allergic diseases,” the authors concluded.
 More people are moving from rural, agricultural settings, which traditionally have had lower rates of allergies, to more urban settings, which have higher levels of air polllution.
More people are moving from rural, agricultural settings, which traditionally have had lower rates of allergies, to more urban settings, which have higher levels of air polllution.—Matthew Ryan, MD
Location, Location, Location
The International Study of Asthma and Allergy in Childhood (ISAAC) has demonstrated a large variation in the prevalence of asthma and rhinitis symptoms in children around the world (Lancet. 1998;351(9111):1225-1232). In particular, the study finds that countries with a very low prevalence of asthma (<5 percent), such as Indonesia, Albania, Romania, Georgia and Greece, also have low prevalence of rhinitis. On the other hand, countries with a high prevalence of asthma (>30 percent), such as Australia, New Zealand and the United Kingdom, have a higher prevalence of rhinitis (15 percent to 20 percent). In countries where the prevalence of allergy and rhinitis is high, “we have seen either a reduction in increase of allergic rhinitis, a plateau in incidence, or a slight reduction in recent years,” Dr. Ryan noted.
The interplay between geography and genetics was the focus of a study of 200,682 men and women (ages 20 to 44 years) seen in 57 centers in Europe, North America, North Africa, India, Australia and New Zealand. Latitude was used as a proxy for ultraviolet exposure (vitamin D), as well as climatic differences responsible for different pollen seasons.
The median prevalence of allergic rhinitis was 22 percent, the authors reported (PLoS Med. 2005;2(10):e294). There was, however, substantial variation across geographic areas. For example, the disorder was far more common the further patients were from the equator. But when the investigators restricted their analysis to Europe, geographical latitude was not a significant factor.
“One intriguing possibility,” wrote lead author Matthias Wjst, “is that a risk factor within language borders might be even more relevant than geographical latitude alone in determining the distribution of allergic diseases—reflecting genetic influences or cultural differences in raising children.”
Impact at Home
In the U.S., it is difficult to determine whether the steep rise in allergic rhinitis over the past 30 years has leveled off. But there is no question that a large number of patients have the disease: It is estimated that allergic rhinitis affects at least 60 million people (see sidebar, “Allergic Rhinitis by the Numbers,” p. 13).
William Reisacher, MD, FACS, FAAOA, assistant professor of otorhinolaryngology at Weill Cornell Medical Center-New York Presbyterian Hospital in New York City, said the prevalence of allergic rhinitis in the U.S. may be even higher. “It affects about 15 percent to 20 percent of the adult population and 20 percent to 25 percent of the pediatric population,” he said.
The toll the disease takes on quality of life is considerable. One survey of 2,500 allergic rhinitis patients and 400 healthcare providers, released in 2006 and endorsed by the ACAAI, found that 59 percent of patients had missed work due to their allergy symptoms. In 2007, a survey of 447 patients with allergic rhinitis by researchers at Kaiser Permanente’s San Diego Medical Center found that about two-thirds of patients with intermittent disease “had some impairment of their professional or daily life as a result of allergic rhinitis” (Allergy. 2007;62 Suppl 85:9-16).
Two other surveys, the Burden of Rhinitis Survey 2004 and the Allergies in America Survey 2006, linked allergic rhinitis to a variety of debilitating co-morbidities, including depression, migraine and asthma.
Treatment and Prevention
Clearly, the stakes are high. Dr. Reisacher said that in most cases, treatment regimens should focus on two primary areas: environmental control and pharmacologic therapy. And, given the large role that people’s increasingly indoor lifestyles play in their disease, limiting the allergenic “load” in the home is crucial.
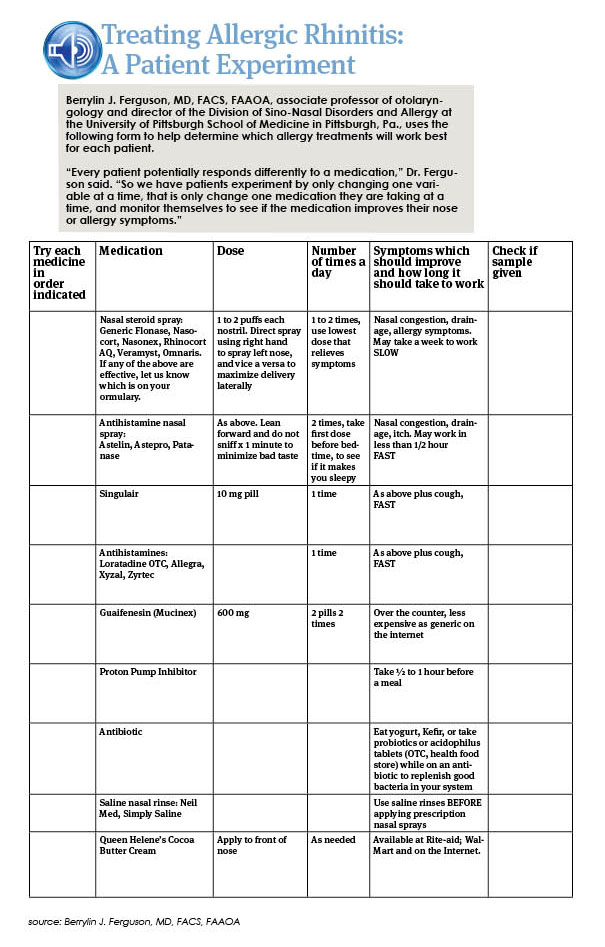
Granted, getting patients to comply with recommendations to address environmental factors that may be contributing to their symptoms “can be a huge challenge,” said Berrylin J. Ferguson, MD, FACS, FAAOA, associate professor of otolaryngology and director of the Division of Sino-Nasal Disorders and Allergy at the University of Pittsburgh School of Medicine in Pittsburgh, Pa.
Environmental controls, therefore, should be directed at things that are “reasonable and practical,” Dr. Ferguson said. For most people with dust mite allergies, for example, the significant exposure is in the bed and pillow. Dr. Ferguson advises patients to purchase breathable mattress and pillowcase covers that are impermeable to dust mites, to wash bedding in hot water once a week and to change pillowcases every three days. “If a patient follows these recommendations, they will reduce their exposure to dust mites by 90 percent, and you avoid the horrendous work of taking every stuffed animal, carpet and drapery out of the room,” she added. (See “Treating Allergic Rhinitis: A Patient Experiment.”)
Dr. Reisacher agrees. “You don’t have to tell patients to completely eliminate everything that they are allergic to in their environment,” he said. “Sometimes, if you can pick one or two things, such as pet dander or mold, that can make a huge improvement.”
Dr. Ryan added one caveat to recommending environmental controls to reduce allergen exposure. In the case of some measures, the scientific proof may be lacking. He cited, as an example, dust mite controls. “Two papers in The New England Journal of Medicine several years ago basically showed that all of the dust mite controls some of us have been advocating don’t really make much of a difference when it comes to reducing overall patient symptoms,” he said. Both of those papers found that allergen-impermeable bed covers, when used as a single intervention for avoiding exposure to dust mites, failed to produce any significant improvement in the symptoms of asthma (2003;349:225-236) or allergic rhinitis (2003;349:237-246).
Such environmental strategies “are not always a miraculous cure for allergic rhinitis,” Dr. Reisacher said. “But they do provide a strong foundation for other interventions, such as pharmacologic and desensitization therapy. The key is patient education. That’s why we spend so much time counseling patients on how to manage their exposures to environmental irritants and allergens, with take-home patient education aids as an important reinforcer.”
Pharmacotherapy and Immunotherapy
While the mainstays of pharmacotherapy are intranasal steroids and antihistamines, unfortunately, “there is no perfect allergy treatment,” Dr. Ryan said. “We don’t have anything that is cheap, works right away, works for every patient and has no side effects.”
Some drugs, given time, can come close to being ideal therapy, at least for some patients, he noted. But in the case of nasal steroids, the trick is often to get patients to comply long enough for the medications to work. “You really have to impress on them that these drugs need to be taken on a daily basis for a period of time before they begin to see symptom relief,” he said. “They have to sort of take it on faith, like a blood pressure pill. You take it to prevent problems further down the road.”
On top of that, Dr. Ryan said, “most allergy patients have symptoms that wax and wane, which makes compliance even more problematic.”
A simple adjuvant to pharmacotherapy is nasal irrigation with a saline solution. “There have been some studies showing that this really works,” Dr. Ryan said. One such study, published this past December, looked at the efficacy of saline nasal irrigation in the treatment of acute sinusitis in children. The randomized, prospective, placebo-controlled trial included 69 patients with acute sinusitis and found that nasal washes significantly improved such symptoms as rhinorrhea, nasal congestion, throat itching, cough and sleep quality in the 40 percent of the children who had allergic disease (Int J Pediatr Otorhinolaryngol 2009;73(12):1696-1701).
Patients who do not improve with environmental controls or pharmacotherapy may turn to immunotherapy. “Of all the tools that we bring to the table, immunotherapy is the only one where we say, ‘This has the potential to cure you,’” Dr. Ferguson said. “The irony is that early exposure to farms and lots of pets—that is, exposure to more bacteria, enterotoxins, or to a dirtier environment—may ultimately protect you from developing allergies. But once you develop allergies, immunotherapy, which exposes you to ever increasing amounts of the allergen, ultimately results in desensitization,” she added.
“One key to success that I would impress on any practicing otolaryngologist is to remember that allergic disease impacts multiple sites in the head and neck that are within the realm of our practice: the eyes, the ears, the nose, the throat, the sinuses—all of these sites can be affected by allergies,” Dr. Ryan said. “All of these can be managed with a carefully considered management plan that includes pharmacologic therapy, some environmental controls, and, in many cases, a lot of patience from the patient and the caregiver.” ENTtoday
Leave a Reply