For example, rates of IEPs continued to be greater than 50% throughout the study, the investigators reported. And yet, in the majority of cases, Dr. Lieu noted, the IEPs did not include any provisions for the children to be tested for hearing loss or to be treated for the condition.
Explore This Issue
March 2014Dr. Lieu contends that a case could be made for 100% of children with UHL getting IEPs that include accommodations for their hearing impairment. But that is not happening, she noted, due to outmoded attitudes towards UHL. “This isn’t viewed as a disability by schools and insurers and other entities,” Dr. Lieu said. “And the logic of that escapes me. As I noted in our 2012 [Laryngoscope] study, having only one functional eye or hand is not challenged as being a disability; why, then, is unilateral hearing loss in kids often not taken seriously?”
Children who come from lower socioeconomic backgrounds and have parents with low health literacy “are the kids I worry about the most, but they also can be the most responsive to interventions,” Dr. Lieu added. She explained that these pressures make it difficult for the children to compensate for their hearing loss on their own. “So, in our practice, we try to fit them with a hearing aid or some other intervention, and we often quickly see improvements in terms of avoiding or mitigating school performance issues and other problems. These kids can benefit an incredible amount from our efforts.”
Dr. Lieu acknowledged that the overall lack of data in this area makes it difficult to issue broad proclamations of which kids with UHL should get which particular type of intervention, and when. But that evidence gap should not cause any hesitation or delay in getting these children some type of help.
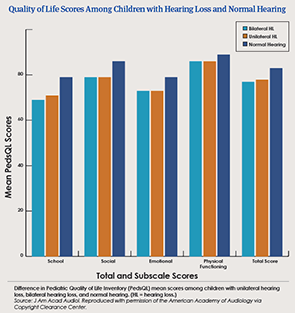
“What the studies do show conclusively is that children with UHL are not doing very well,” she said. “We have published quality-of-life surveys that illustrate this quite clearly [J Am Acad Audiol. 2011;22:644-653; Laryngoscope. 2014;124:570-578]. When you look at the data, you realize that these children are closer to their peers who have bilateral hearing loss than they are to peers with normal hearing. So, how can we not provide them with the best care we have to offer?” (See “Quality of Life Scores among Children with Hearing Loss and Normal Hearing).
Intervene Early—but Proceed with Caution
David M. Baguley, MBA, PhD, head of service: audiology/hearing implants at Cambridge University Hospitals, in Cambridge, England, agreed that although there is a lack of definitive data on managing UHL in children, “that does not justify a lack of action.”
Leave a Reply