Explore This Issue
June 2014
In 2007, the U.S. Food and Drug Administration (FDA) required the labeling on the phosphodiesterase-5 (PDE-5) inhibitors to display more prominently the potential risk for sudden hearing loss associated with all agents in this class (i.e., sildenafil, tadalafil, and vardenafil).
This change came on the heels of a case report of sudden hearing loss in a man taking sildenafil, which in turn prompted an FDA investigation of the post-marketing data of these agents and resulted in the discovery of 23 cases of sudden hearing loss thought to be associated with these agents (J Laryngol Otol. 2007;121:395-397).
Since these initial reports, additional evidence continues to document cases of sudden hearing loss in people taking PDE-5 inhibitors. To date, none of the evidence has established causality, and the mechanism of action remains unclear; however, what does appear evident is support for the recognition that sudden hearing loss may be a real risk in people who take PDE-5 inhibitors. Otolaryngologists should take this into consideration when seeing patients who present with sudden hearing loss.
The Evidence So Far
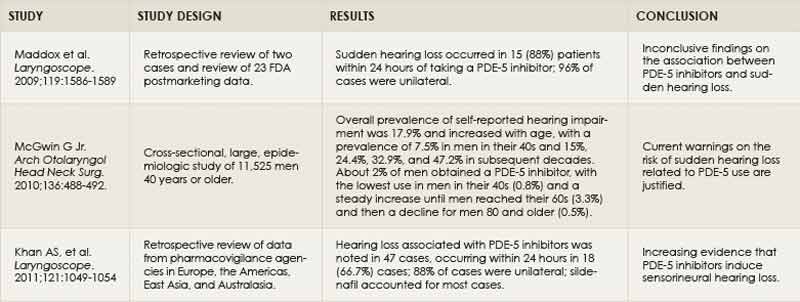
The evidence for an association between PDE-5 inhibitors and sudden hearing loss comes from case reports, one large epidemiological study, and reviews of postmarketing data. In a 2009 report, investigators reviewed two cases of sudden hearing loss from PDE-5 inhibitors along with the FDA postmarketing data in 23 patients (Laryngoscope. 2009;119:1586-1589). Given the retrospective nature of the study and incomplete data from the FDA, as well as the inability to address the potential for confounding variables for sudden hearing loss and comorbidities, the study reported inconclusive findings of the relationship between PDE-5 inhibitor use and sudden hearing loss.
Co-author James E. Saunders, MD, assistant professor of surgery in the division of otolaryngology at Dartmouth Medical School, Dartmouth-Hitchcock Medical Center in Lebanon, N.H., is concerned about the current evidence, saying that it is limited by the retrospective nature of most of the studies and the lack of randomized clinical data. “The problem with case reports is that these drugs are widely used and so there may be reported cases just because the exposure of the drug is so high,” he said.
A report on epidemiological data from more than 11,000 men aged 40 years and older that did adjust for confounding variables concluded that men reporting hearing impairment were more likely to also report using any of the PDE-5 inhibitors (odds ratio [OR] of 2.23, 95% CI, 1.36-3.66) (Arch Otolaryngol Head and Neck Surg. 2010;136:488-492). This association persisted after adjusting for potential confounding variables, including sociodemographic, behavioral, and health-related characteristics.
Although the study found an association between hearing impairment and all PDE-5 inhibitor agents, the only significant association was with the use of sildenafil (OR of 2.05, 95% CI, 1.23-3.43). For the other agents, there was an elevated, albeit nonstatistical, association between tadalafil use and hearing impairment (OR 1.40, 95% CI, 0.49-4.04), and a weaker association with vardenafil (OR 0.88, 95% CI, 0.35-2.22).
According to the author of the study, Gerald McGwin, Jr., MS, PhD, a professor and vice chair in the department of epidemiology in the School of Public Health at the University of Alabama, Birmingham, the study was not able to tease out why sildenafil had the strongest association with hearing impairment, but he added that one possibility was that there were more people using sildenafil. In the study, sildenafil was the most widely used agent (80.3%), followed by vardenafil (20.2%) and tadalafil (12.8%).
He emphasized that the findings of the study need to be placed within the context of the limitations common to all epidemiologic studies. Along with the retrospective nature of the study and the potential for bias with self-reporting, he said that the type of hearing loss associated with the PDE-5 inhibitors (i.e., sudden hearing loss) is relatively uncommon. “You have a sort of needle-in-the-haystack situation,” he said. “You need a large epidemiologic study just to detect what may be a small effect.”
That said, he believes the findings of his study support the FDA warnings. “I think that the FDA warnings are reasonable absent more information,” he said. “There is a risk of some hearing loss and, until there is more epidemiologic data, that warning is warranted.”
In the most recent study, published in 2013, researchers retrospectively reviewed data on side effects of PDE-5 inhibitors from published studies and pharmacovigilance agencies in a number of countries (Laryngoscope. 2011;121:1049-1054). The study found 47 cases of sensorineural hearing loss related to PDE-5 inhibitor use reported in the published literature (n=4) and from pharmacovigilance agencies (n=43). Half of the cases reported were associated with use of sildenafil.
According to the authors, however, the number of cases in their review probably does not reflect the real number of cases of hearing loss related to PDE-5 inhibitors. They mention the potential for an additional 240 cases from clinical and recent FDA reports of adverse events that they were not able to confirm because of incomplete data and case histories. They also note the large variation among the pharmacovigilance agencies they contacted with regard to the level of detail and format of individual adverse event reports, as well as the overall poor response rate from national pharmacovigilance agencies and transnational organizations.
Based on the data they gathered, the authors conclude that there is increasing evidence that the association between the PDE-5 inhibitors and hearing loss is plausible.
Further Investigation
To better understand the association emerging from these studies, investigators have highlighted several issues that need further investigation. One is the physiologic mechanism by which these agents may cause hearing loss, and the other is the need to better understand the temporal relationship between the use of these agents and the onset of hearing loss.
According to Dr. Saunders, there are two main physiologic mechanisms proposed, both of which are implicated in hearing loss and cellular aptosis in the ear. The PDE-5 inhibitors cause a blockage of the breakdown of intracellular cGMP in the hair cell that may potentiate the harmful effects of nitric oxide, or the increased accumulation of cGMP may induce expression of mitogen-activated protein (MAP) kinases and/or nuclear factor-KB (NF-KB). Both the excessive nitric oxide effects and these secondary intracellular regulators have been implicated in hearing loss.
“My personal feeling is that the PDE-5 inhibitor and altered cGMP accumulation probably reduce the ability of the hair cell to respond to a variety of cellular stresses,” said Dr. Saunders, “and that is at least a predisposing factor that renders the ear more likely to develop permanent cellular damage and possibly cell death as a result of a relatively minor stress, such as noise exposure or a minor ischemic event.”
Further research is needed to clarify the mechanism of action of the PDE-5 inhibitors on hearing loss, but all studies to date suggest that the mechanisms set forth are sufficient to establish a plausible association.
Another issue not clearly defined is the temporal relationship between use of these agents and the onset of hearing loss. According to Sujana S. Chandrasekhar, MD, director of New York Otology at the New York Head and Neck Institute, NorthShore-LIJ Healthcare System, and clinical associate professor of otolaryngology at Mount Sinai Medical Center New York City, anecdotal evidence suggests that the onset of hearing loss happens within one to two days of ingesting a PDE-5 inhibitor. This was shown in the 2009 study, of which she was a co-author, which reported that 88% of the cases of hearing loss occurred within 24 hours (Laryngoscope. 2009;119:1586-1589).
Further evidence, she said, comes from the literature on other medications that can cause hearing loss, such as quinine for malaria. “If you take a quinine product for malaria, hearing loss happens within several hours to a day after the dosage,” she said, noting that hearing loss associated with the PDE-5 inhibitors should act in the same time frame. “Given what we’re seeing at the cellular level, it doesn’t make sense that it would take longer for the hearing loss to appear,” she added.
Take Home Message for Otolaryngologists
Despite the unknowns regarding the association between sudden hearing loss and use of PDE-5 inhibitors, there is agreement on the need for otolaryngologists to talk to patients about potential risk.
“When you see a patient with hearing loss, ask them if they’ve used a PDE-5 inhibitor and what the temporal relationship is between the last dose and onset of hearing loss,” said Dr. Chandrasekhar. For patients who are taking PDE-5 inhibitors, and particularly those who do not recover their hearing, she counsels avoiding the use of these drugs.
Dr. Saunders emphasized that he always asks patients about their use of PDE-5 inhibitors if they come in with sudden hearing loss, or with hearing loss that exceeds expectations for the age of the patient and exposure to noise. “I apprise them of the risks of these medications and tell them that the response seems to be individualized, with some people being more susceptible to the effects than others, possibly due to the external stressors such as noise,” he said.
Mary Beth Nierengarten is a freelance medical writer based in Minnesota.
Leave a Reply