Explore This Issue
January 2011A 71-year-old male presented with an approximately 10-year history of a gradually progressive right-sided hearing loss. He had significant noise exposure history having been in the Navy for 30 years, often on aircraft carriers, with his bunk beneath the flight deck. He denied any history of significant childhood ear disease, ear surgery/trauma or family history of hearing loss. He denied any dizziness, imbalance or vertigo. He had no autophony or sound/pressure-related dizziness. On physical examination, both tympanic membranes revealed only mild, diffuse myringosclerosis. He had a shallow retraction pocket superiorly in his right tympanic membrane. Both middle ears appeared well aerated. His audiogram revealed bilateral sloping symmetric sensorineural hearing loss (SNHL) with a large superimposed, low-frequency conductive component on the right. His speech discrimination scores were appropriate, and tympanograms were type A. His acoustic reflexes (500, 1000, 2000 Hz) were present bilaterally.
How would you manage this patient? Go to the next page for discussion of this case.
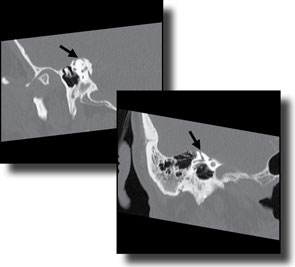
A CT scan of the temporal bones revealed a dehiscence of his right superior semicircular canal. The bone overlying the left superior semicircular canal was thin, but intact. The remainder of the scan was unremarkable. Given that his only symptom was hearing loss, he was offered a hearing aid.
Discussion: The differential diagnosis for a conductive hearing loss is extensive. In this patient, with his findings of mild myringosclerosis and a low frequency conductive loss, the initial consideration was either ossicular discontinuity or otosclerosis. The presence of normal acoustic reflexes eliminates otosclerosis and ossicular discontinuity, however. This key audiological finding led to further investigation with a CT scan. In this situation, the most likely explanation is a mobile third window, i.e., a dehiscent superior semicircular canal. The additional interesting feature in this patient is the absolute absence of vestibular symptoms. Even when the dehiscent superior semicircular canal was recognized on subsequent CT scan and he was re-questioned about vestibular symptoms, he confirmed their absence. Our audiometric testing includes testing for Tullio phenomenon and Hennebert’s signs and symptoms, and he was negative for both. As originally described by Minor and colleagues, the third mobile window phenomenon from a dehiscent superior semicircular canal has the cardinal clinical symptom of pressure or sound-induced dizziness.1 However, further clinical experience has revealed a myriad of associated symptoms attributable to a dehiscent superior semicircular canal, including only conductive hearing loss.2-5
References:
- Minor LB, Solomon D, Zinreich JS, et al. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch Otolaryngol Head Neck Surg. 1998;124(3):249-258.
- Picavet V, Govaere E, Forton G. Superior semicircular canal dehiscence: prevalence in a population with clinical suspected otosclerosis-type hearing loss. B-ENT. 2009;5(2):83-88.
- Ebert CS II, Zanation AM, Buchman CA. Another cause for conductive hearing loss with present acoustic reflexes. Laryngoscope. 2008;118(11):2059-2061.
- Minor LB, Carey JP, Cremer PD, et al. Dehiscence of bone overlying the superior canal as a cause of apparent conductive hearing loss. Otol Neurotol. 2003;24(2):270-278.
- Mikulec AA, McKenna MJ, Ramsey MJ, et al. Superior semicircular canal dehiscence presenting as conductive hearing loss without vertigo. Otol Neurotol. 2004;25(2):121-129.
—submitted by Larry Lundy, MD, associate professor of otolaryngology, Mayo Clinic, Jacksonville, Fla.
Leave a Reply