A billion adults worldwide smoke tobacco, and, according to World Health Organization estimates, their numbers are growing. Six million people die annually from the tobacco habit, and that number is projected to exceed eight million by 2030.
Explore This Issue
October 2013In the United States alone, 43.8 million people still smoke, despite aggressive anti-tobacco campaigns waged by multiple private and government-sponsored organizations over the past several decades. Data from the Centers for Disease Control and Prevention (CDC) suggest that 21.6 percent of men and 16.5 percent of women in the U.S. smoke. Many of those women are in their childbearing years. The Pregnancy Risk Assessment Monitoring System, which monitors changes in maternal and child health indicators in 29 states, puts the overall prevalence of maternal smoking during the last three months of pregnancy at 12.8 percent in the participating states, ranging from a low of 5.1 percent in Utah to 28.7 percent in West Virginia (see map, below).
The list of health hazards associated with smoking continues to grow. According to the CDC, babies born to women who smoke while pregnant have a higher risk of premature birth and low birth weight and an increased risk of sudden infant death syndrome (SIDS), cleft lip or palate, asthma, obesity and cognitive deficits, among other injuries. Now, a new study suggests that hearing loss should be added to this list.
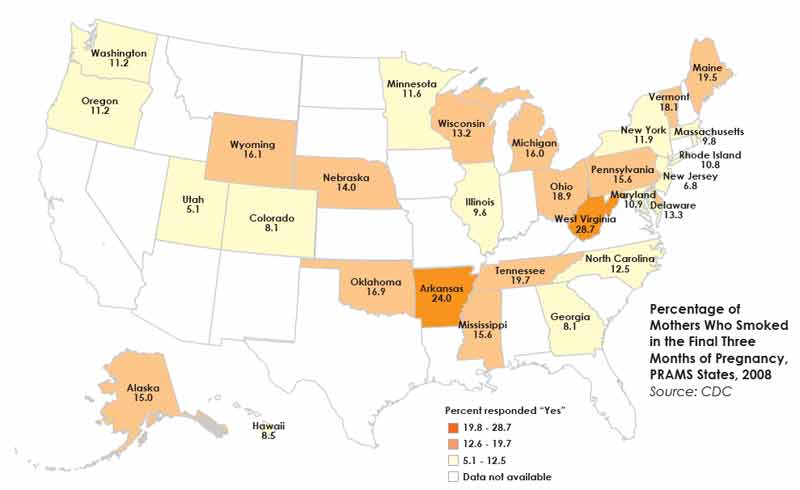
Source: CDC
Setting the Stage
The new findings follow earlier research by the same investigators showing an association between sensorineural hearing loss (SNHL) in adolescents and secondhand smoke (SHS) exposure (Arch Otolaryngol Head Neck Surg. 2011;137:655-662). In that study, the authors referred to data linking prenatal or childhood SHS exposure to numerous health problems including SIDS, asthma and other respiratory tract disorders, and cognitive and behavioral problems, as well as an increased risk of otitis media. The authors also cited evidence that more than 50 percent of adolescents in the United States are exposed to SHS. They hypothesized that secondhand smoke may also have the potential to impact auditory development, leading to SNHL because of its negative effects on in utero development, low birth weight, direct damage to cranial nerve VIII, or brain damage secondary to childhood and adolescent exposure. They tested that hypothesis in a study of young people 12 to 19 years of age.
The researchers drew on data from the 2005-2006 National Health and Nutrition Examination Survey (NHANES), a cross-sectional survey of Americans conducted under the auspices of the CDC. Designed to assess the health and nutritional status of children and adults, NHANES is unique in that it combines in-home interviews and physical examinations. The examinations include collection of blood and urine samples and standard audiometry testing for 12- to 19-year-olds.
Additionally, self-recognition of hearing impairment is assessed by asking people to describe their hearing (sans hearing aid) as excellent, good, having a little trouble, moderate trouble, a lot of trouble or deaf.
The NHANES blood analysis included the measurement of cotinine, a nicotine metabolite that was used as a biomarker for active smoking and exposure to SHS. Adolescents with serum cotinine levels of .05 µg/L to 15 µg/L were defined as exposed to SHS if they denied smoking themselves over the previous five days; those whose serum cotinine exceeded 15 µg/L or reported smoking within the previous five days were considered active smokers, and participants who reported no smoking within the previous five days and had no detectable serum cotinine levels were considered nonsmokers and unexposed to SHS.
Of the 1,533 participants, those considered SHS-exposed had higher rates of bilateral and unilateral SNHL at all frequencies tested, with the differences reaching statistical significance for unilateral low-frequency hearing loss. Overall, SHS exposure was associated with nearly a two-fold increase in the risk of hearing loss in this population. Even worse, lead author Anil K. Lalwani, MD, of the departments of otolaryngology, physiology and neuroscience and pediatrics at New York University Langone Medical Center, and colleagues suggested that the hearing loss might be at an early stage and might progress over time. They also observed higher rates of hearing loss in participants with higher serum cotinine levels, suggesting a possible dose-response effect.
Back to the Womb
These findings prompted the authors to wonder if the negative effects of SHS might begin even before birth: Would a mother’s smoking during pregnancy affect her child’s hearing later on? Once again, they turned to data from NHANES 2005–2006. This time, they included only children between 12 and 15 years of age, because information on maternal smoking behavior was available only for children aged 15 years or younger, while audiometric data were available only for children aged 12 years or more. After exclusion for factors such as incomplete information on maternal smoking or hearing test results, the study sample included 964 adolescents. Of those, 155 (16.1 percent) were born to mothers who had smoked at some time during pregnancy, including 96 (61.9 percent) during the first trimester only. Because of the small sample size, the authors did not determine whether a dose-response relationship existed between maternal smoking and the child’s subsequent hearing loss (JAMA Otolaryngol Head Neck Surg. 2013;139:669-677).
Using the same criteria employed in the earlier study, the investigators identified 400 participants who were SHS-exposed and 432 who were not exposed. Data on smoking activity and cotinine measures were missing in 132 cases, but those individuals were included in the study because there was enough information for the primary analysis, which concerned maternal smoking and hearing loss in the child.
Of the 964 adolescents in the study sample, 92.8 percent of the children of nonsmokers had normal hearing, versus 82.2 percent of those born to smokers.
Children exposed to cigarette smoke in utero were more likely to sustain SNHL at all levels of severity. Most common was mild loss, at 15 to 25 decibels (dB), seen in 5.6 percent of the unexposed children and 11.9 percent of the exposed children. Moderate hearing loss (25 to 40 dB) was seen in 0.9 percent and 4.5 percent of each group, and severe loss (>40 dB) in 0.7 percent and 1.4 percent of each group, respectively (p=0.03 on the Cochrane-Armitage trend test, suggesting the existence of a trend). On bivariate analysis, 7.1 percent of the unexposed and 17.6 percent of the exposed children demonstrated unilateral low-frequency hearing loss (p=0.049). “Adolescents with prenatal smoke exposure had 2.6-fold higher odds of unilateral low-frequency SNHL than unexposed controls,” the authors wrote. The increased risk was independent of SHS exposure after birth. Bilateral and high-
frequency hearing loss were also more common in the children whose mothers smoked during pregnancy, although those differences were not statistically significant.
“This means smoking is dangerous even before you’re born,” Dr. Lalwani told ENTtoday. “There appears to be no period in life when you can escape its effects.” He also pointed out that two-thirds of the mothers who smoked quit during the first trimester, most likely as soon as they learned they were pregnant. “Yet even though the vast majority of women stopped smoking early, we could still detect an effect in the children.”
—Anil K. Lalwani, MD
Unexpected Findings
At least one expert admitted that these findings were somewhat surprising. “I thought this was a well-designed study with a large number of patients, of an important public health problem,” said Clough Shelton, MD, chief of the division of otolaryngology-head and neck surgery at the University of Utah Health Care in Salt Lake City. But he said it was “not on my radar screen at all. That’s why I think it’s important: because I’m sure there are many otolaryngologists like myself who are not following this issue.”
Also surprising was the finding that the biggest difference seemed to be in unilateral hearing loss. “Cigarette smoking is systemic exposure, so you would expect both ears to be affected,” Dr. Shelton told ENTtoday.
“This study provides important information for two reasons,” said Nina Shapiro, MD, director of pediatric ear, nose, and throat at the Mattel Children’s Hospital at the University of California, Los Angeles. “First, we see a hit to the auditory system in utero that manifests itself 12 to 15 years later. That’s something we usually don’t study; generally, we look at the results of maternal habits on infants and newborns. Second, they controlled for secondhand smoke exposure, which is a known risk factor for hearing loss, and they still found more hearing loss among the adolescents who had been exposed in utero.”
It is possible that hearing losses associated with SHS exposure in utero may begin well before adolescence, said Dr. Shelton. “If this effect occurs while the inner ear is forming, then you would expect it to be apparent earlier, and early hearing loss has an impact on a number of things such as speech and language development, which is why this is such an important question.”
Indeed, “it’s very likely that it’s a continuum, meaning that if we were able to check these infants annually or biannually, we might find a progression in their hearing loss,” Dr. Shapiro said. And, “if the group in this study were followed for the next 10 to 20 years, we might see their hearing loss progress even further.”
These findings also suggest that early SHS exposure, be it in utero or during childhood, may be among many environmental factors that, when added together, take a toll on hearing. Unfortunately, said Dr. Lalwani, currently “there’s no good way to tell if there is ongoing deterioration of hearing. These kids may be more susceptible to ear injuries, but right now that’s all conjecture.”
Still, the question resonates. “We sometimes see patients who are more susceptible to noise-induced hearing loss than you would expect; the hearing loss is out of proportion to their noise exposure,” Dr. Shelton explained. “Maybe there’s an environmental factor, such as cigarette smoke, that makes them more vulnerable to this type of noise damage. That’s why I think studying this issue further may be helpful.”
Implications for Otolaryngologists
Otolaryngologists can probably be most helpful in the public message arena, Dr. Shapiro said. “People think about the obvious things associated with smoking, such as pre-term delivery, asthma and all of the respiratory problems, but they don’t really think about hearing as a potential issue. If you have patients who are pregnant, or if you are an otolaryngologist who sees children of women who smoke, I think there needs to be more education on understanding the impact of hearing on child development, language, speech, interaction, school performance, how even changes as subtle as the ones seen in this study may lead to learning issues and memory issues, developmental issues. People who smoke may think their child has normal hearing because she is 3 years old and has passed her hearing test, but she may have already sustained some permanent damage.”
“It’s important to identify risk factors and to ensure that those children are screened,” Dr. Lalwani said. “And, also, to make sure those kids don’t become smokers themselves.”
Leave a Reply