A new guideline from the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) on sudden hearing loss—the first and only U.S. clinical practice guideline on this condition—has garnered mixed reactions from the otolaryngology community.
Explore This Issue
June 2012In keeping with the spirit and letter of these guidelines, the AAO-HNS enlisted the help of a panel of multidisciplinary experts representing otolaryngology, otology, neurology, neurotology, family medicine, emergency medicine and audiology, as well as consumer groups, to review the best evidence currently available on many of the issues pertinent to the clinical management of sudden hearing loss.
The guidelines were presented at the annual AAO-HNS meeting in San Francisco in September 2011 and published last month (Otolaryngol Head Neck Surg. 2012;146:S1-S27).
The guidelines include a detailed explanation of the process by which the panel selected, reviewed and evaluated the current published evidence. Per guideline protocol, each statement is accompanied by an indication of the type of action recommended based on the strength of the evidence. Statements supported by strong evidence are given a “strong recommendation,” and statements supported by evidence with sufficient strength carry a “recommendation,” while statements supported by weaker evidence carry an “optional” directive.
“We don’t want guidelines to be cookbooks; rather, we want them to be resources that people can look to for best practices for treatments based on the best evidence available,” said Robert J. Stachler, MD, division chief of otolaryngology at Henry Ford Hospital, clinical associate professor at Wayne State University in Detroit, Mich. and lead author of the guidelines. Although Dr. Stachler said he believes most of the issues covered in the guidelines will not raise too much debate, he did highlight a few that have generated some discussion. The following issues refer to patients diagnosed with sudden sensorineural hearing loss (SSNHL) as opposed to conductive hearing loss.
Optional Corticosteroid Use and Hyperbaric Oxygen
Statement eight, which states that initial treatment of SSNHL with steroids is optional, may be most surprising to clinicians who see these patients.
According to Sujana Chandrasekhar, MD, director of New York Otology and vice-chair of the guidelines, most of the guidelines panel went into the review process with a bias toward using oral systemic steroids for initial treatment, because it reflects standard current practice by most clinicians who treat SSNHL. The current evidence on the efficacy of initial oral steroids, however, was not strong enough to warrant a recommendation, she said. “We are not saying that we recommend against initial treatment with steroids; we are saying it is optional,” she said.
For David R. Friedland, MD, PhD, professor and vice-chair of otolaryngology and communications sciences at the Medical College of Wisconsin in Milwaukee, making initial oral steroid use optional is problematic, particularly when this practice is coupled with the other initial treatment that the panel rated as optional: hyperbaric oxygen (statement nine).
“For the most part, hyperbaric oxygen is not used in the United States, and, for the most part, initial use of oral steroids is commonly used in this country,” he said. “To give those two treatments equal weight in a guideline is ignoring current practice and is not acknowledging the health care system in this country.”
The inclusion of hyperbaric oxygen as optional initial therapy was also highlighted by two other sources weighing in on these guidelines. John C. Li, MD, an otologist, neurotologist and otolaryngologist in private practice in Jupiter, Fla., said that he was surprised by the inclusion of hyperbaric oxygen because it is not commonly available and can be very expensive. He has seen costs billed to insurance companies as high as $2,300 per session.
“I personally have not had much luck with hyperbaric oxygen therapy,” Dr. Li added, noting that he no longer uses it based on the poor cost-benefit ratio.
Similarly, Lorne S. Parnes, MD, professor of otolaryngology at the University of Western Ontario, London Health Sciences Centre, London, Ontario, said that “emphasizing hyperbaric oxygen therapy was a disservice, as it is extremely costly and not available in most centers.” He also said it was an oversight of the guidelines panel to leave out a recommendation on the use of combined oral and IT corticosteroid therapy as an initial treatment.
Dr. Chandrasekhar acknowledged that hyperbaric oxygen is not widely used in the U.S., is not approved by the U.S. Food and Drug Administration for use as initial steroid therapy for SHL and is very costly. However, she said that it was included as optional initial therapy for SHL in these guidelines because of its wide use outside the U.S. and evidence from trials that support its use.
According to Dr. Stachler, no one expected to find support for hyperbaric oxygen as an initial option for treatment, but the evidence from overseas could not be ignored.
Salvage Intratypanic Steroids
According to Dr. Friedland, statement nine, which recommends the use of intratympanic (IT) steroids as salvage, is questionable. It doesn’t make sense to say that initial therapy with oral steroids is optional but that IT steroids as salvage is recommended, he said.
“Biologically, it is not consistent. Why would a steroid work a month later and not immediately?” he said. He added that his main contention is the different level of ratings given, with the weaker optional rating for initial steroid use and the stronger recommended rating for IT salvage steroids. He questioned the strength of the evidence for IT steroids, saying that the evidence is “extremely poor.”
“The issue I have for this particular recommendation is that most of the studies that showed an effect or improvement with IT salvage steroids only showed an improvement of about 12 decibels on average,” he said. “I don’t think that is clinically significant to warrant such a strong recommendation for using IT salvage steroids for treatment of [sudden hearing loss].”
He also emphasized that the use of IT steroids as salvage is not current standard practice, which means that the guidelines, if followed, will change current practice. He cautioned that this may be a difficult recommendation for private practitioners to follow because many are not trained in or comfortable with using IT steroids, or for those who are not able to get adequate preparations.
Dr. Chandrasekhar, who said that others have also expressed concern over the perceived inconsistency between the statement that initial oral steroid use is optional but salvage IT steroids are recommended, said the guidelines are evidence-based and that readers need to read the guidelines from a scientific perspective.
“The data is very compelling for salvage IT steroids,” she said. “This makes sense clinically. The reality is we see people all the time who come to us after they’ve received a treatment for a diagnosis they don’t have, or who have received insufficient steroid treatment or who have not responded to appropriate treatment, and then we treat with salvage IT.”
She also said that offering IT steroids is well within the parameters of what general otolaryngologists do and emphasized that she trains many otolaryngologists every year in the use of this procedure during her course on sudden hearing loss at the annual AAO-HNS meeting. Otolaryngologists who are not comfortable doing this procedure or those who don’t have access to the necessary preparations can refer patients to a trained specialist, she said.
In addition, she said that discussion of this option is recommended based on the current evidence, but nothing in the guidelines prevents any physician from exercising his or her educated, clinical judgment.
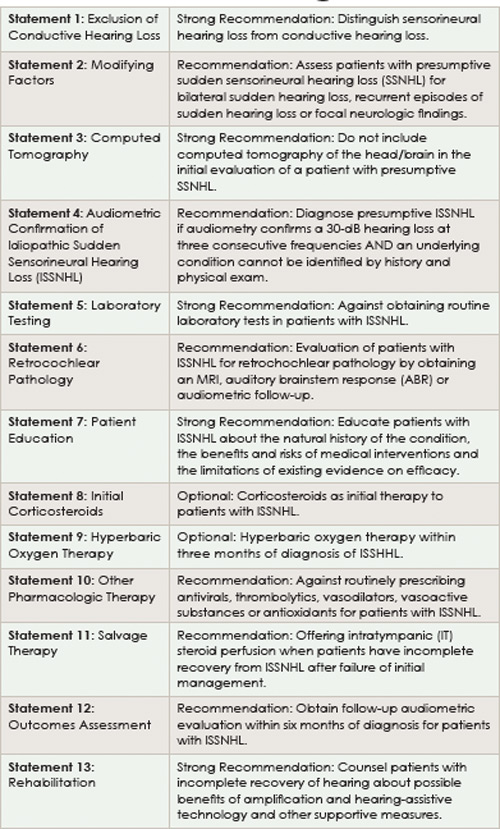
Statements supported by strong evidence are given a “strong recommendation,” and statements supported by evidence with sufficient strength carry a “recommendation.”
Change Clinical Practice or Raise Necessary Questions?
Underlying this discussion of specific statements reported in the guidelines is the overall question of what defines a guideline and what constitutes its main purpose.
“Our goal is to change clinical practice in that we want to encourage the provider to know the literature better and engage in a good dialogue with the patient, “said Dr. Chandrasekhar. She said, for example, that it’s important to make patients aware of some of the issues surrounding oral steroids and hyperbaric oxygen, because patient preference plays a big role in both treatment options.
In addition to affecting clinical practice, she said she believes the guidelines will lead to a secondary goal, which is to drive clinical research.
“We used to think that oral steroids was the gold standard for first-line therapy, and we thought it would be unethical to run a trial that included a non-steroidal treatment arm,” she said. “Now, the evidence suggests that it is probably quite in the boundaries of ethics to do at least a short trial including a non-steroidal treatment arm.”
Dr. Li said he supports the need for a unified approach to diagnosis and treatment and agrees overall with the guidelines, with several caveats. Among these is the use of some caution in adhering to the recommendation to minimize tests. Although he agrees that offering MRI scans seems wasteful, given the fact that over 90 percent of scans are negative, he generally offers it and discusses it as an option because of medical-legal issues. “Unfortunately, what can come with guidelines are new gold standards that can create medico-legal issues for people who either knowingly or unknowingly fail to follow these guidelines,” he said.
Dr. Friedland said the current guidelines represent a good review of the literature and can be seen as a good guide for clinical decision making, but he doesn’t think they should be defined as a guideline. “A guideline to me implies a standard of care, what clinicians should and are expected to do if faced with a patient. It puts a physician in a position of justification if they deviate from the guidelines,” he said. “The problem I have with this guideline is that a majority of the evidence used to support treatment recommendations for [sudden hearing loss] is not useful or valid, and to formulate a guideline based on that is dangerous.”
Dr. Stachler said the guidelines are not set in stone and should be considered recommendations based on the best evidence. “There are times that a physician may not follow a recommendation for various reasons, and it is important that the guidelines are not seen as punitive,” he said. He also noted that all guidelines are updated every five years and acknowledged the need for more data to clarify the role of steroids as upfront treatment.
Leave a Reply