October 1, 2013 should be on the mind of every physician in the U.S. That is the day when a new diagnostic coding system will be instituted, the first such change since 2003. The implementation’s aftermath is predicted to be anywhere from a normal day at the office to financial Armageddon.
Explore This Issue
December 2011“It is imperative that practices begin to think strategically and figure out what needs to be done and how to pay for it,” said Rhonda Buckholtz, CPC, CPMA, CENTC, vice president of ICD-10 education and training for the American Academy of Professional Coders (AAPC).
In January 2009, the U.S. Department of Health and Human Services released new standards for adoption of the International Classification of Diseases, Tenth Revision (ICD-10). ICD-10 CM (Clinical Modification) will be used in all health care settings. ICD-10 PCS (Procedure Coding System) is used only in the inpatient hospital setting. After October 1, 2013, the old ICD-9 codes will not be usable for billing in most health care settings.
New Codes for New Times
According to the Centers for Medicare and Medicaid Services (CMS), the transition to ICD-10 is occurring because ICD-9 produces very limited data about patients’ medical conditions and hospital inpatient procedures. In addition, the three to five-digit structure of ICD-9 limits the number of new codes that can be created. Over the years many ICD-9 categories have become full, making it even harder to capture the full nature of diseases in the U.S. The ICD-10 transition will include seven-character codes.
“ICD-9 is completely outdated,” Buckholtz said. “Not only is there a need for more codes, but [there is] a lack of space for new codes.”
This means that the 17,000 different codes currently used in ICD-9 will grow to more than 140,000 when ICD-10 is fully implemented. In addition, the new codes require more specificity in coding and documentation. One code currently used for acute otitis externa, for example, becomes 28 potential codes.
“We are the U.S. and the king of supersizing,” Buckholtz said. “We have taken our clinical modification of ICD-10 to a higher level than other countries. For example, in Australia they have around 16,000 codes, while Canada and Germany have under 20,000.”
In addition, the U.S. is the only country using the ICD-10 system for billing purposes. Most of the other nations use it mainly for epidemiological reasons. Canada is among those countries that use it only in hospitals.
Financial Concerns
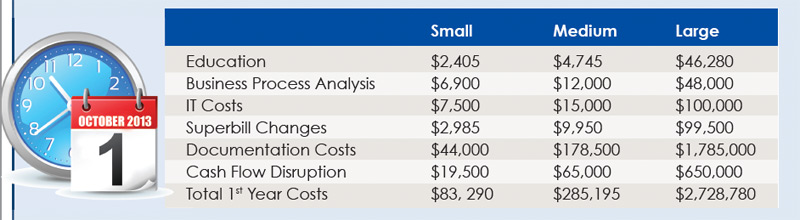
Implementation will be costly. A white paper developed for America’s Health Insurance Plans in 2006 suggested a total cost of between $3.2 and $8 billion. A 2008 study by Nachimson Advisors, LLC, estimated that a typical small practice of three physicians can expect costs of more than $83,000 by the time the changeover is complete. A practice of 10 providers may spend as much as $285,000 to fully implement ICD-10.
In addition to having to come up with the money to pay for computers, software and staff training, companies have very real financial worries about timely payments during the changeover.
There is no consensus developing about how smoothly payments will flow in early October 2013. Credible scenarios have included everything from no discernable difference to checks being held up for three months or more. Over the constellation of payers, it is likely that some will be better prepared than others.
“Practices definitely should be trying to put money in the bank and arranging lines of credit,” said Kim Pollock, RN, MBA, CPC, a consultant with KarenZupko & Associates, Inc., a Chicago practice management consulting and training firm. “You might be entirely ready, but if there are glitches at the payer’s end, you won’t get paid. Payments are not entirely in the practice’s control.”
Robert Tennant, a senior policy advisor with the Medical Group Management Association (MGMA) in Washington, D.C., suggested that practices consider putting off major capital expenses in the two to three months leading up to the compliance date. Think hard about the immediate need for a new piece of diagnostic machinery, expansion of the office or any other big cash expenditure in the run-up to ICD-10.
 “ICD-9 is completely outdated. Not only is there a need for more codes, but [there is] a lack of space for new codes.”
“ICD-9 is completely outdated. Not only is there a need for more codes, but [there is] a lack of space for new codes.”
—Rhonda Buckholtz, CPC, CPMA, CENTZ
How Specific?
Another financial concern will be payer policies. Even CMS is unable to give guidance about the level of specificity that will be required.
“Both systems have a code for unspecified sinusitis,” Tennant said. “One health care plan says 82 percent of sinusitis claims use that code. We are concerned that there is no clarity on whether plans will continue to pay ‘unspecified’ claims at the same rate, a lower rate or reject them.”
Even when there is more transparency on how plans will handle this, individual practices may still not know what to expect when a specific patient walks in the door.
“You will probably have to know not only which insurance company, but the specific insurance product involved,” Tennant said. “Each plan and each product could potentially have a different level of required detail.”
Another major change will be in the area of charting.
“Documentation for ICD-10 is a huge issue,” Buckholtz said. “Readiness assessments show there is not enough information to assign a code to the highest level of specificity in 35 percent of the cases. It tends to open a doctor’s eyes when we ask if they are prepared to live on 65 percent of their income.”
The biggest difference will be in the granularity of the codes. There will be codes specific to which side of the body is affected, whether this is a first encounter or ongoing treatment and whether a condition is chronic or acute. Buckholtz pointed to two different injury codes, one for being struck by a turkey and another for being pecked by one, to show how far ICD-10 will drill down in the encounter. To be properly claimed, this much detail must be reflected in charting.
Superbills may be a thing of the past in many practices. Depending on the case mix, a replacement superbill may turn out to be 10 pages or more.
Code sets for ICD-10 are already available through CMS. One suggestion is that providers sit down with the new codes and existing charts to see if their current documentation supports the more in-depth requirements of ICD-10. If not, then they should begin to document patient encounters at the higher levels required so that they can get into the habit before October 2013.
Provider Productivity
Provider productivity issues must also be considered. More documentation time will be required, which may mean that a provider sees fewer patients, especially during the early days. Tennant pointed to a Robert E. Nolan Company report that anticipates that the average doctor will see the equivalent of a four-patient-per-day decrease in productivity. Tennant thinks the reduction could be permanent.
An AAPC white paper describes the experiences of Vancouver General Hospital following Canada’s implementation of a new system in 2000. Initially, the hospital’s average coding time per record doubled, as did its payment turnaround, while its coding backlog went from 64 days to 139. More than 10 years later, productivity has not yet returned to pre-implementation levels.
There may be some parallels with the experiences of practices when their electronic medical records (EMR) systems went online.
“When we went to our EMR system three years ago, I had to spend a tremendous amount of time learning how the system worked and less [time] actually talking to patients,” said Michael Setzen, MD, clinical associate professor of otolaryngology at New York University School of Medicine and a physician in private practice in Great Neck, N.Y. “They weren’t happy that I was in the room with them using the computer. Overall, the volume of interactions with patients will be decreasing. For how long is the major question.”
Audit Workflows
Another thing practices should undertake soon is a top-to-bottom workflow audit.
“We are telling clients they should inventory the practice looking for any use of ICD-9 codes on superbills, forms, policies, reports and payer information,” said Pollock. “Run a frequency report to determine your top 25 or so diagnosis codes. Then you can map the ICD-9 codes to the draft ICD-10 codes now. Look for areas of insufficient documentation to choose the appropriate ICD-10 code. Then, when the final code set is released in October 2013, you are a step ahead in ensuring your documentation will support the new codes.”
Every part of your practice will need to be assessed. At the front desk, privacy policies will most likely need revisions, as will patient encounter systems. The practice managers will have to look at all policies and procedures associated with a disease code, disease management, tracking and the Physician Quality Reporting Initiative while also reviewing and updating all vendor and payer contracts. Nursing will be involved in changes to order forms and prior authorizations. Even the laboratory will need to be more precise in how it documents its work.
Training
One of the most significant costs to the practice will most likely be staff training. Not only will the coding and billing staffs need to be educated, but the physicians themselves will need training.
Buckholtz said the AAPC will be working both with local chapters and at the national level to provide educational programs (See “Resources for Getting Your Practice Ready”). “We already have implementation boot camps available for early planning. As it gets closer to time, we will be offering specialized courses for coders and physicians,” she said.
She cautioned against starting training too early. Training that begins more than six to nine months before the new codes are used will likely be forgotten by the time it is needed. There is also little need to spend time working with codes until October 2012.
“A lot of things have to come together to make this work,” said Tennant. “It is a challenging cascade for the organization, starting from the education of administrative staff through upgrading or replacing practice management and billing system software, up to the training of physicians themselves.”
Working with Vendors
Major changes will also be needed in your practice management systems, billing software and even your EMR. In some cases, the practice may simply need to update its current systems. Other practices may need to buy new programs and update hardware.
Practices should start by talking to their computer system vendors. Their schedules for updating programs will be one of the main variables. Find out from your vendor when your current systems will be upgraded or replaced to handle the new codes and workflow processes.
For some, upgrades may be included as part of system maintenance. Those who find that their current version can’t be upgraded will have to buy a new software suite.
The new year brings the implementation of Version 5010, a protocol making the changes that will allow computers to talk to each other using the larger ICD-10 codes. Despite CMS requirements, some Medicaid programs have announced that they will not be ready by the January 1, 2012 target date. In early November, CMS announced that it would not initiate enforcement action for non-compliance with the 5010 standards until March 31, 2012. With some groups missing this first major deadline, there are bound to be stragglers when ICD-10 starts.
Even if CMS and all plans actually change their systems on time, ICD-9 will not be going away any time soon. It will still be used for patients seen on or before September 30, 2013, even if billed afterwards. ICD-9 will continue to be the standard for workers compensation and disability claims.
“There has to be a mindset in every practice that this isn’t going to be a simple transition,” said Dr. Setzen. “It is not that we bill ICD-9 today and ICD-10 tomorrow.”
After the early planning and research to get ready for the change, the hard work will begin in late 2012 and continue into 2013. After the new code set is frozen in October 2012, the actual implementation of computer system changes, coding training and transition to ICD-10 can begin.
In early 2013, practices should be ready to start testing the new systems. It is important to make sure all claims actually get to billers and clearinghouses. Practices must also follow claims until they are successfully adjudicated by the payer to make sure there are no glitches further down the line. There may be one last minor tweaking of the codes just prior to implementation.
Every practice should find out when its clearinghouse will be ready to accept test batches of claims to see how well the systems work together. They should ask all payers the same process questions. These test runs should take place as soon as possible so that there is time to find and correct problems.
All three experts interviewed stressed that practices must get specific answers to these questions in writing. Vendors who are unwilling or unable to do so may not be ready. Practices encountering this problem should consider changing vendors.
“With ICD-10, it is possible for you to do everything right and still not get paid,” said Buckholtz. “What happens upstream is very important to the practice, too.”
Plan Ahead
Although the experts see no need to panic at this time, they do stress that now is the time for practices to start to gather information on ICD-10. (See “Resources for Getting Your Practice Ready,”)
Denise Buenning, MsM, director of the Administrative Simplification Group (ASG) in CMS’ Office of E-Health Standards and Services, said ICD-10 will go ahead on schedule.
“In the final rule, we extended the proposed compliance date from October 1, 2011 to October 1, 2013 to accommodate industry feedback that [indicated that] more time would be needed for systems and business process transitions to ICD-10, and there is stakeholder support for CMS adhering to that timeline,” she wrote in an e-mail to ENT Today.
“At this time, practices should be settling on a point person and begin early planning,” Tennant said. “Start looking at timelines, talking to vendors about their plans to provide upgrades, find where ICD-9 codes are currently being used so you know where ICD-10 codes will need to go and develop budgets and training schedules. Basically, find out all you can without spending a dime.”
Resources for Getting Your Practice Ready

There are several resources available, many free of charge.
- American Academy of Otolaryngology—Head and Neck Surgery
entnet.org/Practice/ICD-10.cfm
Multiple pages of information on ICD-10 implementation that address issues specific to otolaryngology, including a slide set from the presentation at the 2010 annual meeting.
- CMS
Information from both the Centers with links to other, non-governmental resources.
- American Health Information Management Association
Information on training available from the association, information on authorized resellers and a list of white papers that can be purchased, as well as others that are available for free.
- Healthcare Information and Management Systems Society
Lists of information on planning, financial considerations, gathering human resources and budget considerations.
- AAPC
Touches on most general aspects of implementation, with an additional concentration on training staff and physicians on coding issues.
- Medical Group Management Association
Focused more on the practice manager side of implementation.
Leave a Reply