Laurie McCombs, 53, has dealt with sinus problems nearly all of her adult life. Clogged sino-nasal passages made it difficult for her to breathe at night, and the congestion caused morning pressure headaches. Over-the-counter and prescription antihistamines muted her symptoms but did not address their cause. At the age of 40, she decided to take the advice of friends who had experienced relief with acupuncture. Now McCombs follows the advice of the acupuncturist, who diagnosed her with allergies to dairy products and yeast, by limiting her intake of breads and milk products. She also continues to take loratadine and has found saline irrigation with the neti pot helpful in clearing her sinuses.
Explore This Issue
April 2010Studies of complementary and alternative medicine (CAM) use in the specific setting of chronic rhinosinusitis (CRS) have been modest to date. Jon Newton, MD, and colleagues from the department of otolaryngology, head and neck surgery at the Aberdeen Royal Infirmary in Scotland surveyed patients admitted to their tertiary care center for elective otolaryngologic surgery and found that 63 percent of patients had used some form of complementary or alternative therapy (J Otolaryngol Head Neck Surg. 2009; 38(3): 355-361). What do these trends mean for otolaryngologists and their patients? Do any of these remedies show efficacy, and how should physicians solicit disclosure and provide patients with guidance regarding their use? Experts interviewed by ENT Today weighed in.



Turning to Other Solutions
It’s the chronic nature of rhinosinusitis that makes complementary therapies appealing, said Richard J. Harvey, FRACS, associate professor of rhinology/skull base surgery at St. Vincent’s Hospital in Sydney, Australia. “When conditions are chronic—and rhinology is full of them—the concept of control of a chronic inflammatory airway condition, rather than cure, is very challenging for patients,” he said.
Michael D. Seidman, MD, FACS, director of the division of otologic/neurotologic surgery and medical director of wellness for Henry Ford Health System in Detroit, Mich., said physicians are much more adept at healing acute conditions. “But for patients with chronic sinusitis who keep trying different treatments—antibiotics, surgery—and nothing’s working, it’s reasonable to consider some of the integrative medicine strategies,” he said.
But Do They Work?
Since David Eisenberg’s landmark studies in the 1990s (JAMA. 1998;280(18):1569-1575), physicians have become increasingly aware of their patients’ use of remedies outside of the allopathic armamentarium. CAM encompasses a broad range of techniques, from acupuncture, massage and yoga, to herbal products and aromatherapy. Dr. Harvey applies a scale of “plausible to preposterous” when educating his patients about CAM. Among the most plausible of late: saline irrigation, delivered by a variety of means, including the neti pot, which comes from a yogic/Ayurvedic healing tradition. Dr. Harvey is principal author of The Cochrane Collaboration review of nasal saline irrigations for symptoms of CRS (Cochrane Database of Systematic Reviews. 2007;3;CD006394). He and co-authors found reliable evidence that nasal irrigation as an adjunctive treatment “is likely to improve symptom control in patients with persistent sino-nasal disease.”
Another large-scale review of the existing literature of CAM in rhinitis and asthma, conducted by the ARIA (Allergic Rhinitis and its Impact on Asthma) initiative concluded that the therapeutic efficacy of CAM treatments is not supported by currently available evidence (J Allergy Clin Immunol. 2006;117(5):1054-1062). Other systematic literature reviews, conducted by the Department of Complementary Medicine headed by Edzard Ernst, MD, PhD, FRCP, FRCPEd, at the University of Exeter in the U.K., have come to similar conclusions. One review found that although there were “promising” results for herbal products such as butterbur extract and several Chinese herbal medicines, the results were limited due to paucity of data, small sample size and lack of confirmatory rigorously designed randomized controlled trials (RCTs) (Ann Allergy Asthma Immunol. 2007;99(6):483-495). Another review noted limited evidence for the efficacy of herbal products, although it cited “encouraging” evidence for the use of bromelain (pineapple extract) as an adjunctive in acute rhinosinusitis (Otolaryngol Head Neck Surg. 2006;135(4):496-506).
Pros and Cons
Patients’ choices to explore complementary therapies draw varying opinions from otolaryngologists. “I’m very happy for my patients to explore complementary medicines, as long as I believe that the complementary therapy isn’t at great time or financial expense for them,” Dr. Harvey said. Although he is extremely cautious about the use of herbals prior to surgery, Dr. Harvey gives patients handouts about selected herbal products and vitamins, such as grape seed extract and vitamin C, that can help ease their rhinitis symptoms.
Richard F. Lockey, MD, president of the World Allergy Organization and professor of medicine, pediatrics and public health and the Joy McCann Culverhouse Chair in Allergy and Immunology at the University of South Florida College of Medicine in Tampa, gives unequivocal advice to his patients: “I am a scientist first and everything else second,” he said. “Except for nasal lavage, I’m not open to any of that. I just tell patients like it is: ‘We used to call it quackery, but now we call it alternative medicine.”
“I think skepticism is appropriate,” said Dr. Seidman, who holds a degree in human nutrition and is also director of the Henry Ford Health System’s Center for Integrative Medicine and has studied nutraceuticals since 1981. “To those who say, ‘There are no studies to verify that,’ the answer is, you have to know where to look for those studies.” He cites, for instance, work done by the German Commission E (http://cms.herbalgram.org/commissione.index.html), which publishes monographs on herbal medicines, showing that Echinacea purpurea is effective in up-regulating T-cell phagocytosis.
Dialogue Is Essential
Whether or not physicians agree with their patients’ choices to explore complementary therapies, one thing is certain: Careful communication with patients is essential. In the Aberdeen study, only 43 percent of patients who used CAM had informed their physicians of this fact. A 2006 survey conducted by the National Center for Complementary and Alternative Medicine (NCCAM) and the American Association of Retired Persons (AARP) found that almost 70 percent of respondents had not told their physicians about CAM approaches they had tried.
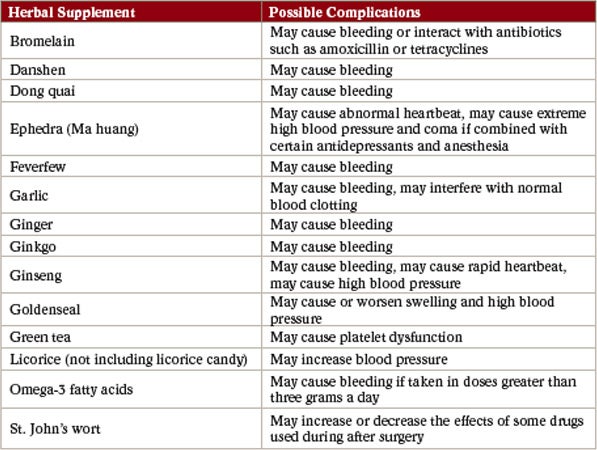
If patients are taking herbal supplements, safety issues arise. Many herbal remedies possess significant pharmacological activity and can cause potential adverse effects and drug interactions (Arch Facial Plast Surg. 2001;3:127-132). Dr. Seidman points out that St. John’s wort, commonly used to treat mild depression, is especially dangerous with inhalation anesthetics. Dr. Harvey follows the recommendations of the American Society of Anesthesiologists, which advises discontinuation of any herbal products two weeks prior to surgery (see “CAM and Endoscopic Sinus Surgery,” p. 16).
Jordan Josephson, MD, FACS, director of the New York Nasal and Sinus Center in New York City, thinks it behooves physicians to take their patients’ preferences into consideration. “Whether we like it or not,” he said, “patients are going to continue to pursue alternative therapies. Patients will not tell you that they use CAM therapies if they think you will not approve. This puts you and the patient in jeopardy, because there might be interactions between those therapies and the ones you are offering. We really all need to join forces and try to educate patients,” he said.
Gretchen Henkel is a medical writer based in California.
ONLINE EXCLUSIVE: Treating Allergic Rhinitis: A Patient Experiment
Berrylin J. Ferguson, MD, FACS, FAAOA, associate professor of otolaryngology and director of the Division of Sino-Nasal Disorders and Allergy at the University of Pittsburgh School of Medicine in Pittsburgh, Pa., uses the following form to help determine which allergy treatments will work best for each patient.
“Every patient potentially responds differently to a medication,” Dr. Ferguson said. “So we have patients experiment by only changing one variable at a time, that is only change one medication they are taking at a time, and monitor themselves to see if the medication improves their nose or allergy symptoms.”
| Try each medicine in order indicated | Medication | Dose | Number of times a day | Symptoms which should improve and how long it should take to work | Check if sample given |
| Nasal steroid spray: Generic Flonase, Nasocort, Nasonex, Rhinocort AQ, Veramyst, Omnaris. If any of the above are effective, let us know which is on your ormulary. | 1 to 2 puffs each nostril. Direct spray using right hand to spray left nose, and vice a versa to maximize delivery laterally | 1 to 2 times, use lowest dose that relieves symptoms | Nasal congestion, drainage, allergy symptoms. May take a week to work SLOW |
||
| Antihistamine nasal spray: Astelin, Astepro, Patanase | As above. Lean forward and do not sniff x 1 minute to minimize bad taste | 2 times, take first dose before bedtime, to see if it makes you sleepy | Nasal congestion, drainage, itch. May work in less than 1/2 hour FAST | ||
| Singulair | 10 mg pill | 1 time | As above plus cough, FAST |
||
| Antihistamines: Loratadine OTC, Allegra, Xyzal, Zyrtec | 1 time | As above plus cough, FAST |
|||
| Guaifenesin (Mucinex) | 600 mg | 2 pills 2 times | Over the counter, less expensive as generic on the internet | ||
| Proton Pump Inhibitor | Take ½ to 1 hour before a meal | ||||
| Antibiotic | Eat yogurt, Kefir, or take probiotics or acidophilus tablets (OTC, health food store) while on an antibiotic to replenish good bacteria in your system | ||||
| Saline nasal rinse: Neil Med, Simply Saline | Use saline rinses BEFORE applying prescription nasal sprays | ||||
| Queen Helene’s Cocoa Butter Cream | Apply to front of nose | As needed | Available at Rite-aid; Wal-Mart and on the Internet. |
Source: Berrylin J. Ferguson, MD, FACS, FAAOA
Leave a Reply