Minimally invasive OSIA 2 System reduces the risk of signal attenuation and skin complications, which were limitations of previous percutaneous and older transcutaneous devices.
Minimally invasive OSIA 2 System reduces the risk of signal attenuation and skin complications, which were limitations of previous percutaneous and older transcutaneous devices.

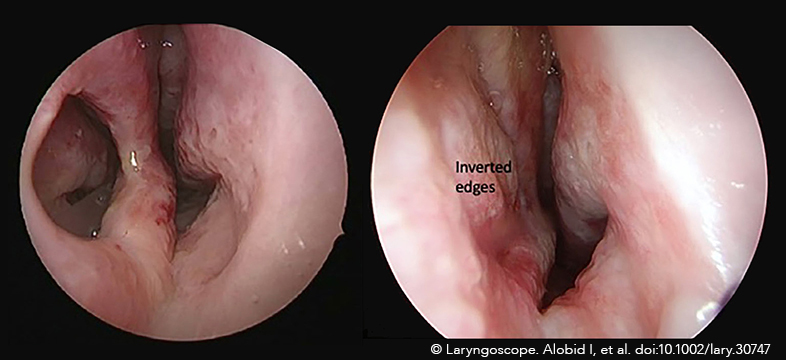
It is commonly accepted that early diagnosis and timely and effective joint reduction are the keys to treating arytenoid dislocation. In this article we take a look at a novel five-step reduction technique.
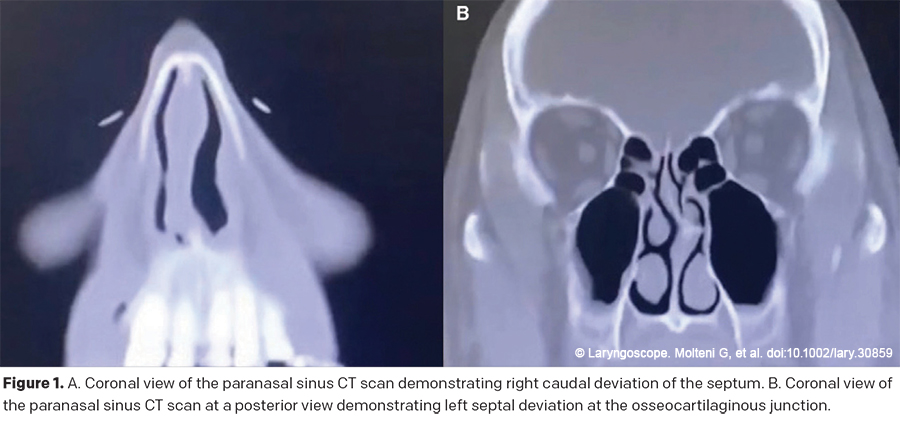
This article provides a detailed description of a dynamic endonasal columellar strut placement technique, as well as its clinical relevance and impact on patients after they have undergone routine septoplasty.
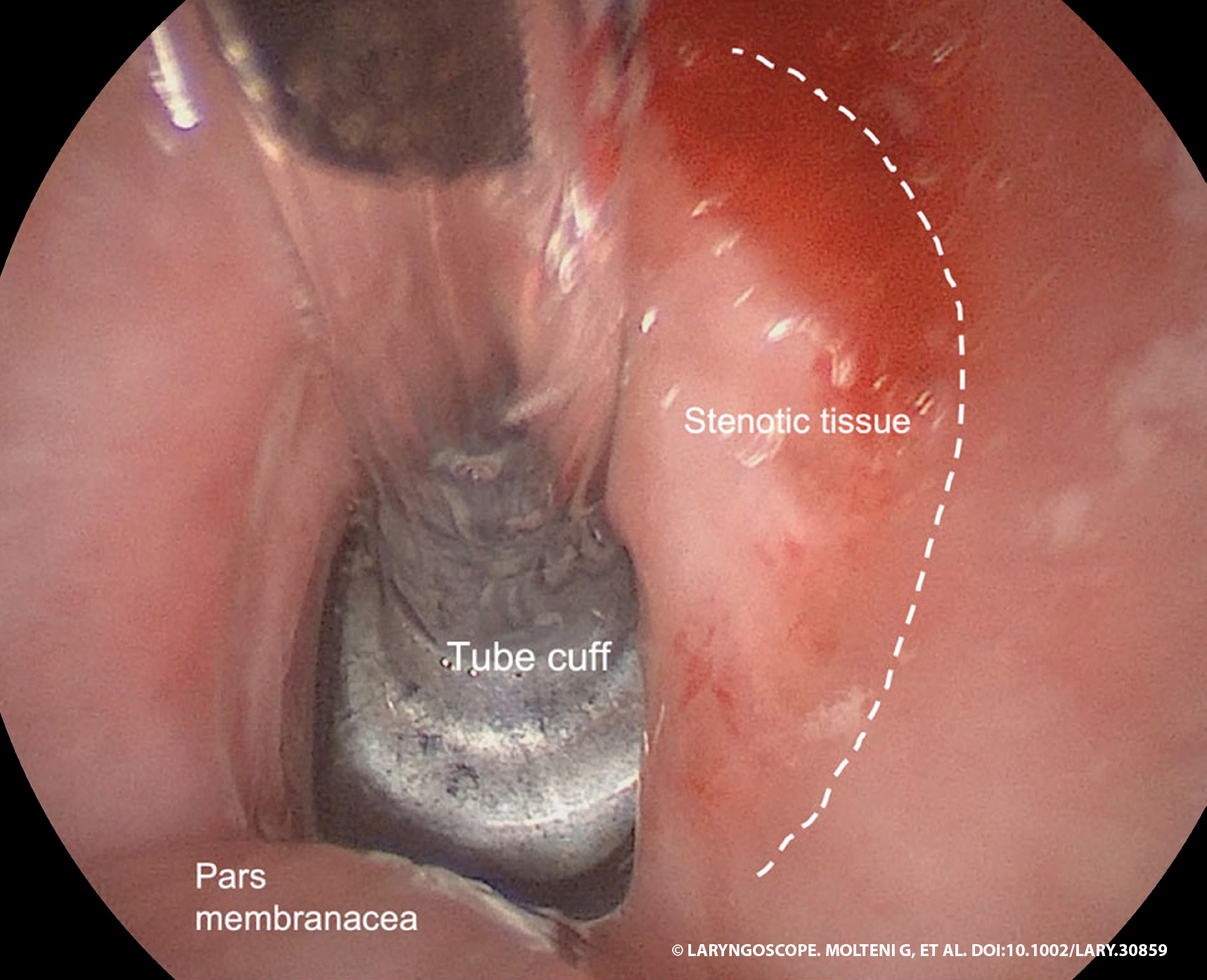
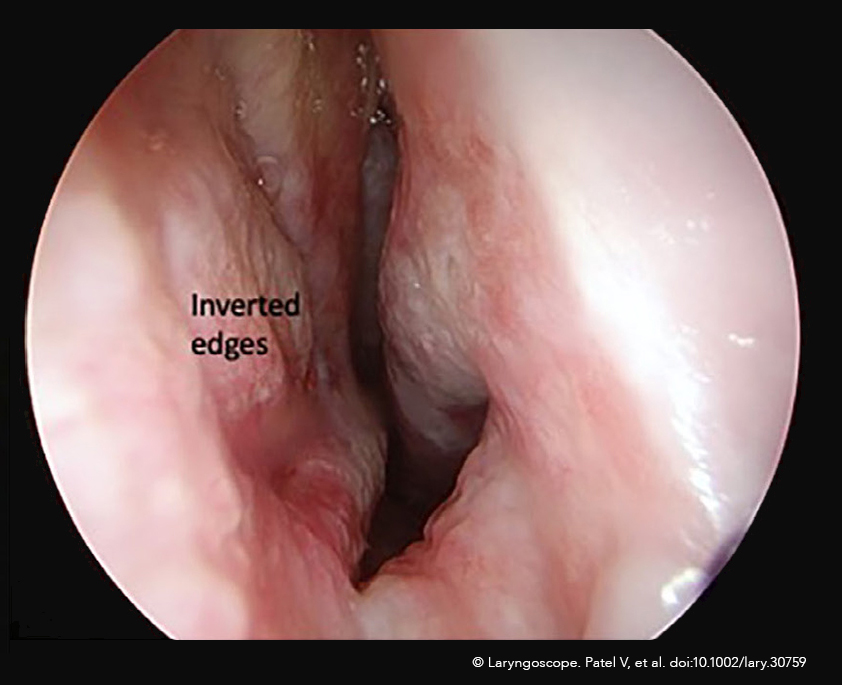
Up to 12% of all COVID-19 patients may need intensive care unit admission for severe interstitial pneumonia, with possible long-term endotracheal intubation for mechanical ventilation, but prolonged endotracheal intubation can lead to mucosal injury and inflammation, granulation tissue formation, perichondritis, and subsequent stenotic scar tissue development.

Should transoral options be limited or unavailable, recent reports have demonstrated success in closing oroantral fistulae with different intranasal mucosal flaps.
A recent survey demonstrated that respondents had a similar preference for the endoscopic and external rhinoplasty approaches, followed by the endonasal approach.
Adoption of the ICG-endoscopic technique has decreased operative times, improved surgeon ergonomics, increased confidence in preserving neurovascular anatomy, and increased resident participation given superior visualization projected onto a 4K screen.

Rapid additive manufacturing of a superlight obturator for large oronasal fistula in pediatric patients are considered more comfortable, more cost-effective, and precise than conventional impression techniques
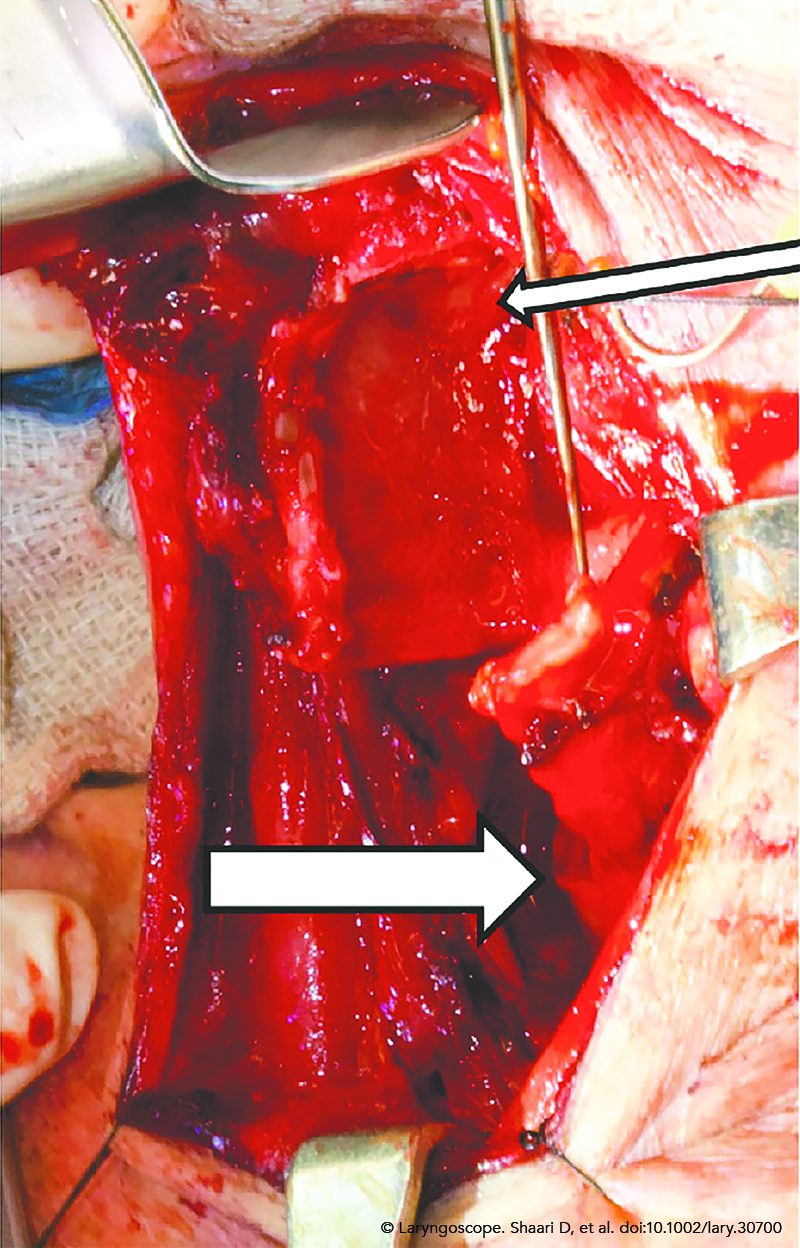
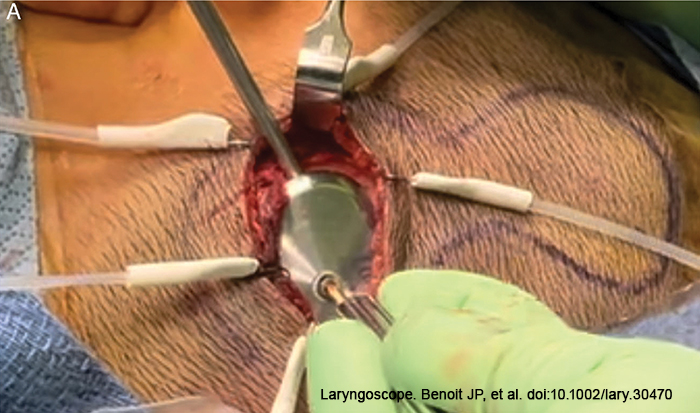
Novel sternocleidomastoid flap augmentation of tracheal reconstructive technique for invasive thyroid cancer is designed to incorporate the sternocleido-mastoid muscle flap directly over the tracheal suture line to minimize the risk of anastomotic complications.

This novel method of positioning the patient for SCD repair allows for optimal head rotation, requires less set-up and patient manipulation, does not require surgical pins, and allows the surgeon to maintain an ergonomically ideal posture during microdissection.