Explore This Issue
January 2012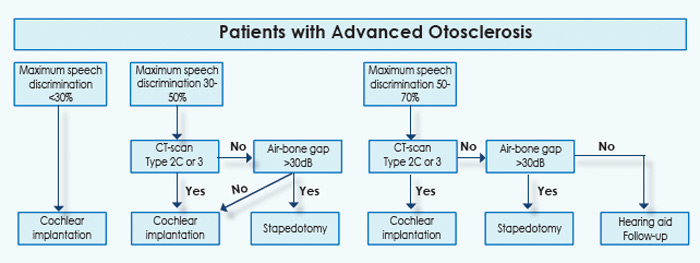
Can stapes surgery—a technique that hasn’t changed fundamentally in 20 years, according to Dr. Smullen—really be the first option for many patients with severe otosclerosis? “I do cochlear implants on a weekly basis, so I am fully capable and willing to recommend implants if I feel they are warranted,” she said. “But the big gun is just not always the best choice.”
Dr. Merkus said he agrees that “going with stapes surgery first is the prudent thing to do for many patients with advanced otosclerosis,” adding that the algorithm supports that approach for selected patients. But he stressed that in rare cases of severe bone remodeling, “it is not advised to perform a stapedotomy, because by postponing CI surgery, you could be creating a very difficult CI surgery in future as the bone remodeling continues.”
David S. Haynes, MD, FACS, professor of otolaryngology, neurosurgery, and hearing and speech sciences at Vanderbilt University School of Medicine in Nashville, Tenn., said the algorithm developed by Dr. Merkus and his colleagues “is a reasonable approach; diagnosing and staging advanced otosclerosis can be extremely difficult, so a systematic method for doing that is welcome, especially in the absence of any consensus guidelines on how to manage these patients.”
With regard to the CT component of the algorithm, “they are correct in relying on those findings to guide their interventions,” Dr. Haynes said. “But I would add a caveat here: CT scans don’t always give you the whole story with these patients; it can underpredict disease progression. That’s why we sometimes order an MRI, which gives a more complete picture of what’s going on. In fact, it sometimes will allow us to choose the better ear for our surgery of choice in a particular patient.”
Dr. Haynes echoed Dr. Smullen’s point that aggressive efforts should be taken to preserve a patient’s natural hearing. “That’s why when we perform a CI, we do a round-window insertion and use ‘soft surgery,’ which is a minimally invasive approach to implantation,” he said.
Because of such refinements to CI, “the trend in many clinics over the past 15 years is to rely more on the technology of CI to provide hearing to a wider range of patients, as opposed to stapedectomy. In fact, implant technology has progressed to the point where, along with our abilities to fine-tune the programming of the CI processor, the implant technology can override what we can provide with stapes surgery alone in these cases of far-advanced cochlear otosclerosis.”
Leave a Reply