Dr. Reisacher agrees. “You don’t have to tell patients to completely eliminate everything that they are allergic to in their environment,” he said. “Sometimes, if you can pick one or two things, such as pet dander or mold, that can make a huge improvement.”
Explore This Issue
March 2010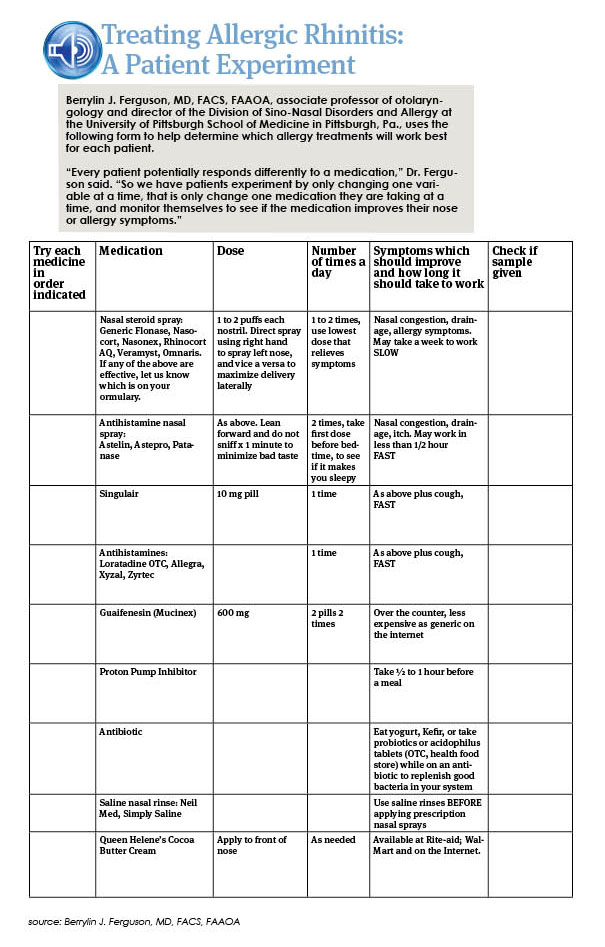
Dr. Ryan added one caveat to recommending environmental controls to reduce allergen exposure. In the case of some measures, the scientific proof may be lacking. He cited, as an example, dust mite controls. “Two papers in The New England Journal of Medicine several years ago basically showed that all of the dust mite controls some of us have been advocating don’t really make much of a difference when it comes to reducing overall patient symptoms,” he said. Both of those papers found that allergen-impermeable bed covers, when used as a single intervention for avoiding exposure to dust mites, failed to produce any significant improvement in the symptoms of asthma (2003;349:225-236) or allergic rhinitis (2003;349:237-246).
Such environmental strategies “are not always a miraculous cure for allergic rhinitis,” Dr. Reisacher said. “But they do provide a strong foundation for other interventions, such as pharmacologic and desensitization therapy. The key is patient education. That’s why we spend so much time counseling patients on how to manage their exposures to environmental irritants and allergens, with take-home patient education aids as an important reinforcer.”
Pharmacotherapy and Immunotherapy
While the mainstays of pharmacotherapy are intranasal steroids and antihistamines, unfortunately, “there is no perfect allergy treatment,” Dr. Ryan said. “We don’t have anything that is cheap, works right away, works for every patient and has no side effects.”
Some drugs, given time, can come close to being ideal therapy, at least for some patients, he noted. But in the case of nasal steroids, the trick is often to get patients to comply long enough for the medications to work. “You really have to impress on them that these drugs need to be taken on a daily basis for a period of time before they begin to see symptom relief,” he said. “They have to sort of take it on faith, like a blood pressure pill. You take it to prevent problems further down the road.”
On top of that, Dr. Ryan said, “most allergy patients have symptoms that wax and wane, which makes compliance even more problematic.”
A simple adjuvant to pharmacotherapy is nasal irrigation with a saline solution. “There have been some studies showing that this really works,” Dr. Ryan said. One such study, published this past December, looked at the efficacy of saline nasal irrigation in the treatment of acute sinusitis in children. The randomized, prospective, placebo-controlled trial included 69 patients with acute sinusitis and found that nasal washes significantly improved such symptoms as rhinorrhea, nasal congestion, throat itching, cough and sleep quality in the 40 percent of the children who had allergic disease (Int J Pediatr Otorhinolaryngol 2009;73(12):1696-1701).
Leave a Reply