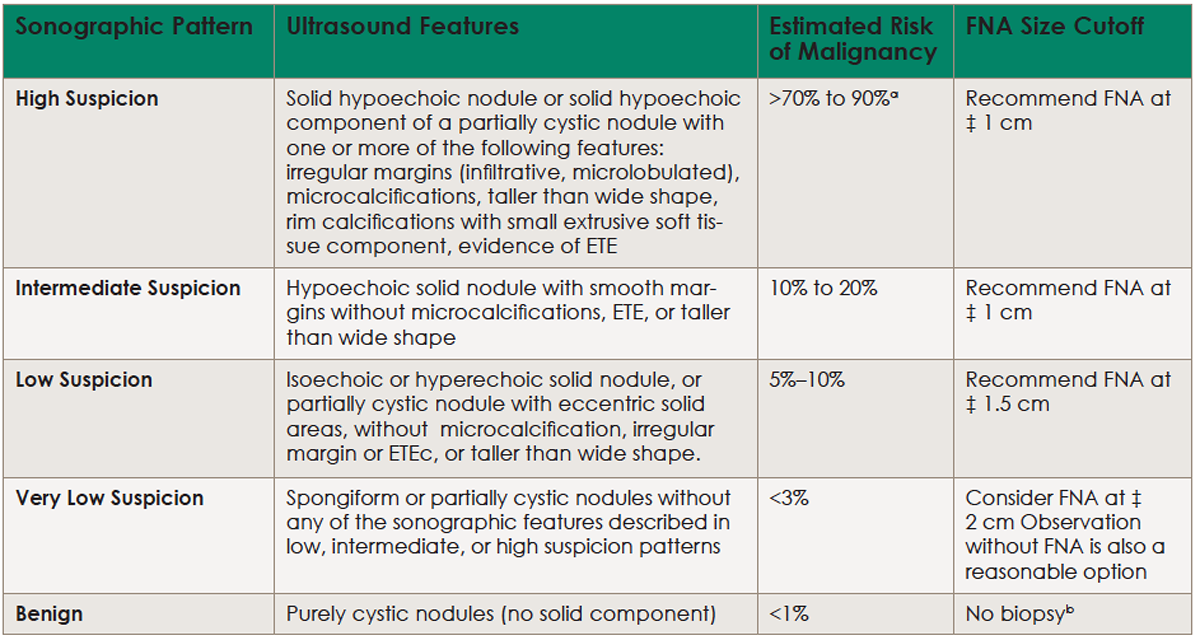
(click for larger image) Table 1. Sonographic Patterns, Estimated Risk of Malignancy, and Fine Needle Aspiration Guidance for Thyroid Nodules
Ultrasound (US)-guided FNA is recommended for cervical lymph nodes that are sonographically suspicious for thyroid cancer.
aEstimate is derived from high volume centers; overall risk of malignancy may be lower given the interobserver variability in sonography.
bAspiration of the cyst may be considered for symptomatic or cosmetic drainage. ETE, extrathyroidal extension.
Updated Information
One reason for the update is that there have been significant scientific advances in evaluation, biopsy criteria and result interpretation, molecular markers, and benign nodule management since the previous guidelines were released in 2009, leading to revised recommendations in all of these areas.
Explore This Issue
June 2016An advantage of these expanded recommendations is a greater ability to fine-tune diagnosis and personalize treatment decisions based on patient preference and clinical context. “With indolent growth pattern and generally excellent prognosis associated with the majority of these cancers, these numbers beg questions about how much diagnostic work-up and treatment is necessary for thyroid nodules and well-differentiated thyroid cancer,” said Dr. Zafereo.
There are rarely sudden shifts in clinical practice, and the ATA guidelines are no exception to that, Dr. Zafereo added. There are some general trends that are more apparent in the 2015 version, however. “These guidelines endorse a generally measured approach to biopsy of thyroid nodules and treatment of differentiated thyroid cancer,” he said. “For example, small and sonographically low-risk nodules may not be recommended for biopsy.”
“It’s certainly been an evolution,” said Dr. Tufano. “The 2015 guidelines are the third iteration, and, each time, there has been a greater attempt to personalize and tailor treatments to individual patients, rather than putting everyone in the same box. Clinicians have to be more thoughtful about what treatment we’re going to render, and the expanded information allows patients to better participate in making the determination of what’s best for them.”
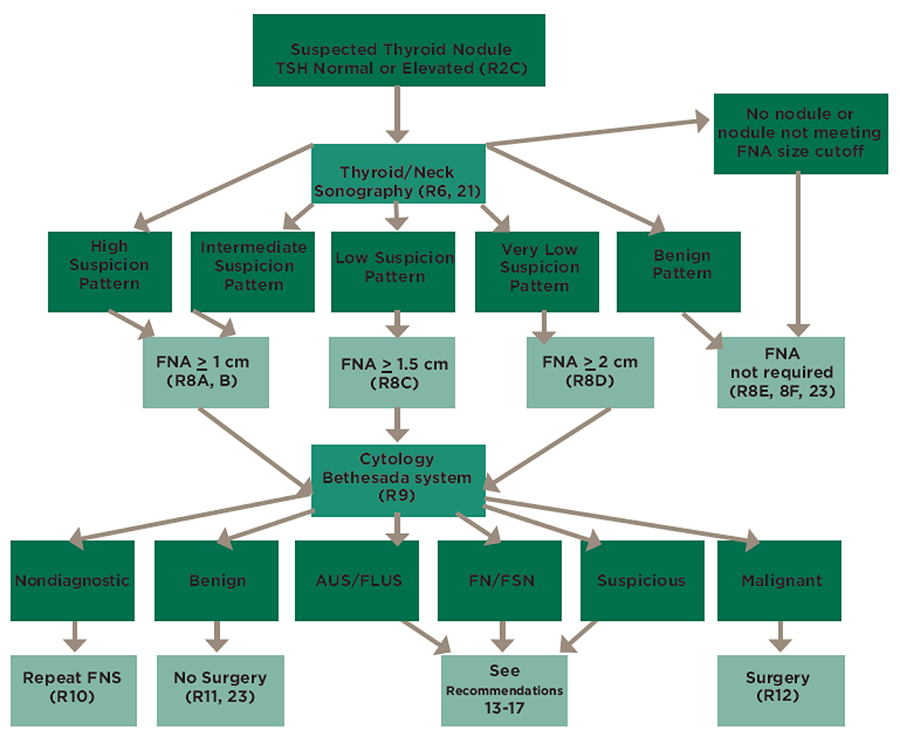
(click for larger image) Figure 1. Algorithm for evaluation and management of patients with thyroid nodules based on US pattern and FNA cytology; several algorithms such as this one are available in the guidelines for quick reference to aid clinicians.
These guidelines can also serve as a starting point for increased dialogue with patients and colleagues about therapy options. “We are seeing a high number of patients with thyroid cancer, and the numbers continue to increase each year,” added Dr. Tufano. “However, the overwhelming majority are small differentiated thyroid cancers; in that circumstance, we feel that since we’re not able to provide objective prognostication on what a tumor will or will not do, we want to make sure we’re very thoughtful about each treatment.”
“There is a general ‘less is more’ trend in terms of surgical management and adjuvant radioactive iodine therapy for low-risk, well-differentiated thyroid cancer,” said Dr. Zafereo. “Ten years ago, many more patients were undergoing total thyroidectomy and postoperative radioactive iodine for well-differentiated thyroid cancer, whereas evidence-based current clinical practice has shifted to more thyroid lobectomies and avoidance of radioactive iodine for smaller well-differentiated thyroid cancers because of excellent long-term outcomes even with lesser therapy.