Based on the structural mechanisms described above, academic and non-academic hospitals grew, and we’ve churned out higher proportions of fellows, who have increasingly gone to the competition of academic centers. In some markets this may have a negative feedback effect of pulling subspecialty referrals away from academic centers and decreasing training numbers, with the possible effect of suppressing training growth. Or, the opposite could happen: these hospitals are in alternative locations, build a critical mass of subspecialists, start their own residencies, and increase supply further. Since our GME growth is currently expanding at historic rates, this remains more theoretical, but it’s important to follow from a competition and supply perspective.
Explore This Issue
July 2022What remains clear is that, from the consumer perspective, competition currently isn’t geared toward maximizing value. As we jockey with each other in this inefficient market, we haven’t been exploring our workforce in detail and publishing this examination regularly for all to see so that market participants can make more efficient decisions for themselves. And we’ve been forgetting about where the real threat comes from in competition: not from the organization down the street, but from the outside—and that disrupts the normal way of things for all of us.
Future Workforce Design
To craft a more efficient healthcare system with more accountability and competition based on consumer value, we need systemic change that arises from lobbying efforts. Site-neutral payments and, more importantly, consumer price transparency should be the norm. We expect that of any other market interaction and service provided—why are we special?
Transparent outcome data, with appropriate controls, that patients care about should replace the current quality mandates put out by CMS. These transparency changes allow for more efficient allocation of capital— patients will go where they perceive the value is, and workforce changes will follow. Also, if taxpayers are footing the bill for PSLF, it should be curtailed to apply only to employment in access-challenged settings, regardless of the employer’s 501(c)(3) status. But these items aren’t under our control as a specialty.
As noted in part II of this series, we have a transparency problem—we don’t put out nuanced workforce information on a routine basis for market participants to digest. Just as a more value-transparent healthcare system allows for a more efficient patient allocation of capital, more transparent workforce information allows for a more efficient allocation of labor.
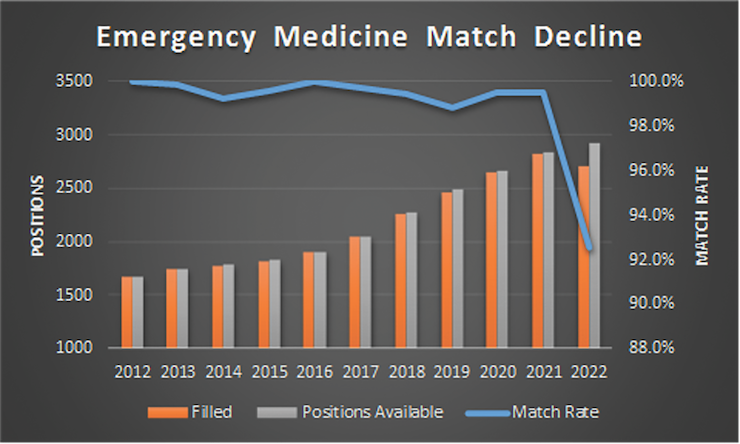
Figure 2