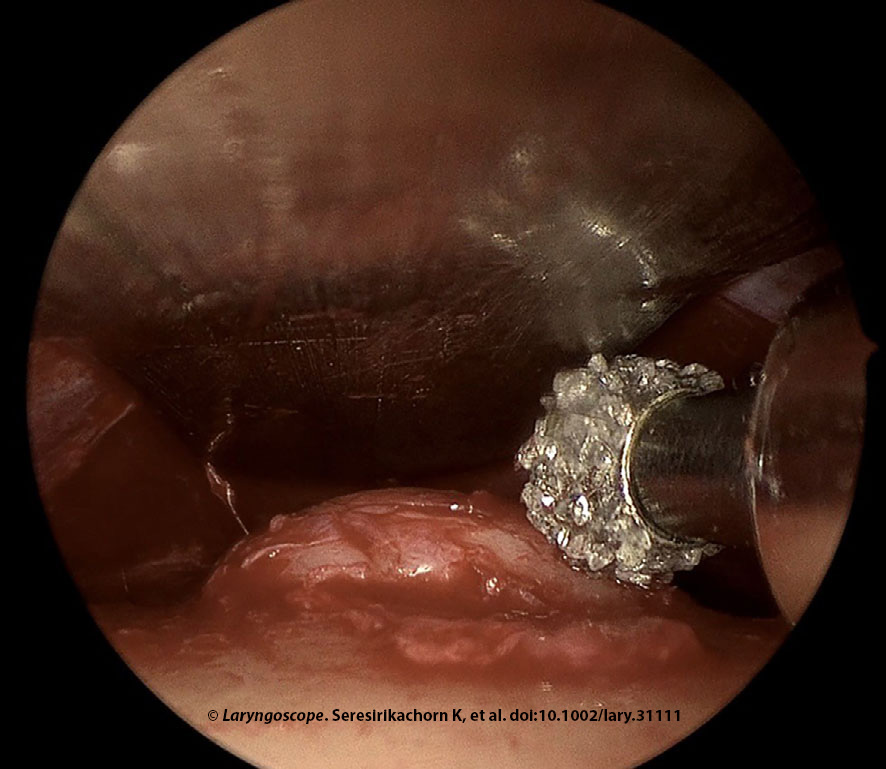
Figure 1. Endoscopic forehead osteoma removal was done in a 49-year-old female with an 11 mm left forehead osteoma. Drilling is shown here.
The forehead osteoma removal was performed with a 4-mm 15° diamond burr at 30,000 revolutions per minute, along with irrigation and suction system under 0° endoscope visualization. Irrigation and suction were critical for drilling to reduce heat and clean the surgical field. The surgeon held the 0° endoscope above the drill, whereas the assistant held the malleable retractor. The uneven frontal bone surface was recontoured with drilling. The ethmoid curette was used to smooth any minor irregularities after drilling (Figure 1). Finally, irrigation with normal saline was performed to clean the operative field and ensure that all bone debris was removed. The wound was closed using absorbable sutures (5-0 coated Vicryl and 5-0 Plain Gut). The forehead was compressed with an elastic bandage for three to five days postoperative.
Explore This Issue
January 2024Postoperative Care
Patients were managed via day surgery. Amoxicillin/clavulanic acid was given for 10 days, and prednisone was given at 25 mg daily for seven days to reduce swelling.
RESULTS
Nine patients (48.9 ± 10.1 years, 100% female) were assessed. The osteoma diameter was 11.7 ± 3.5 mm. Multiple osteomas were present in 29%. All patients had complete removal of forehead osteoma (100% [95% CI: 66.4%–100%]) and success in restoration of contour (100% [95% CI: 66.4%–100%]). The follow-up was 24.8 ± 19.1 months. There were no early (0% [95% CI: 0%–33.6%]) or late (0% [95% CI: 0%–33.6%]) surgical morbidities.
Similar outcomes have been reported with complete removal and excellent cosmesis. The technique described utilizes familiar drills and endoscopic equipment for the otolaryngologist. The subperiosteal dissection and osteoma removal steps were performed via endoscopic visualization. Although performing osteoma removal without endoscope visualization using osteotome and hammer instrumentation has been described (Formos J Surg. 2015. doi:10.1016/j.fjs.2015.04.001), the endoscope provides precise drilling and limits soft tissue dissection. Additionally, this skill set is very familiar to otolaryngologists.
The risk of supraorbital or supratrochlear nerve injury, and subsequent paresthesia, are often minimized by the subperiosteal approach, the high incision, and small port access. In our series, the entire dissection and tumor removal were performed via a single remote port. Multiple port approaches for endoscopic removal of forehead osteoma, attributed to the complexity arising from an excessively narrow inter-instrument angle that impedes manipulation, have been described in the literature but are not required. Otolaryngologists are familiar with endoscopic visualization via a single port, similar to that used for endoscopic sinus or ear surgery.