“The prevailing viewpoint of surgeons when they are referred a patient with a smaller than 1 cm thyroid cancer or microcarcinoma is to feel obligated to remove it, despite thinking that the nodule should not have been biopsied in the first place,” he said. This is considered standard of care as recommended by the current American Thyroid Association (ATA) guidelines; however, Dr. Morris emphasized that this recommendation has created a disconnect in thinking among otolaryngologists and other physicians managing thyroid cancer. The disconnect, he said, is that the guidelines say that it is unnecessary to biopsy small (1 cm or less) thyroid lesions, because cancers this size are believed to be clinically insignificant; however, if these small lesions are biopsied, surgeons feel compelled to treat them as clinically significant (i.e., perform a thyroidectomy).
Explore This Issue
May 2014He emphasized, however, that just because it is now known that a small thyroid nodule is cancer does not change the fact that it is a low-risk cancer with generally indolent behavior.
Based on this fact, he and his colleagues at Memorial-Sloan Kettering currently give patients who present with small papillary thyroid cancers the option of surgery or active surveillance. Active surveillance usually consists of following the patient with an ultrasound every six months for two years and once a year after that. He and his colleagues offer this to patients with cancers up to 1.5 cm in size. Over 80% of patients who have been offered active surveillance at Memorial Sloan-Kettering chose that option over surgery, he said.
R. Michael Tuttle, MD, an endocrinologist at Memorial Sloan Kettering Cancer Center, is a lead investigator on a long-term observational study looking at outcomes of about 100 enrolled patients who chose active surveillance. All patients in the study are 18 years of age or older, with 1-cm lesions confined to the thyroid and no abnormal lymph nodes as detected by ultrasound. To date, he said, the patients have been followed for two to three years, and about 90% of patients have no change in their lesions. In 10% of patients with slowly growing tumors, surgery was performed. Dr. Tuttle emphasized that these data mirror what the Japanese have been reporting for years (see Table 2).
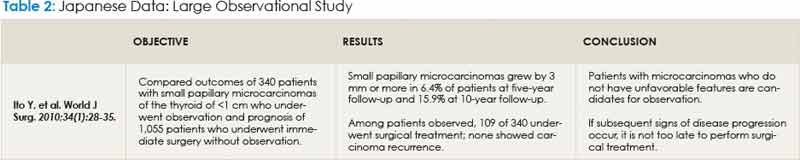
“We are very nicely reproducing the Japanese experience, and if this works over the next 100 or so patients, I think it will give us all the comfort in properly selected patients to say that we don’t need to rush to surgery and we can watch these lesions,” he said.
Leave a Reply