Obstructive sleep apnea (OSA) affects an estimated 2 to 4 percent of adults and is associated with multiple morbidities, including hypertension, congestive heart failure, myocardial infarction, diabetes and neurocognitive impairment. In addition to these significant health consequences, the effects of OSA can extend to an increased risk for motor vehicle accidents and an impaired quality of life (BMJ. 2008;336:44-45; Laryngoscope. 2012;122:1878-1881; Sleep. 2007;30:461-467).
Identifying and treating patients with this disorder is imperative, but how do we determine that we have, in fact, successfully improved the health of individuals for whom surgical intervention was deemed necessary?
Surgical Options
Once a diagnosis of OSA is made, most patients receive the front line of OSA treatment: continuous positive airway pressure (CPAP) devices. In most cases, sleep quality is improved quickly, and daytime sleepiness is reduced. But CPAP use has a number of side effects. The mask can cause a claustrophobic feeling, and the airflow can result in a dry, sore mouth and nasal congestion. These discomforts are significant enough for many patients to stop using the device. Patient compliance is a major obstacle to successful CPAP therapy, which is defined as reducing the apnea-hypopnea index (AHI) to 5 or less, effectively “normalizing” the patient’s breathing during sleep.
Should CPAP therapy fail, either through lack of compliance or simple lack of effectiveness, surgery may be indicated. Surgery is a second-line OSA treatment, used strictly when CPAP or mandibular advancement devices have not delivered relief. In some cases, surgery can be considered as a first-line treatment if the patient exhibits an obvious anatomical abnormality that could be blocking airflow to the lungs. In these cases, correcting the anomaly could successfully eliminate the problem.
Surgical interventions for OSA depend on the anatomical issue being addressed. Procedures include:
- Maxillo-mandibular advancement (MMA): skeletal surgery that advances the soft palate, tongue base and suprahyoid musculature and stabilizes the alterations with screws, plates or bone grafts;
- Uvulopalatopharyngoplasty (UPPP): excision of the tonsils and posterior soft palate and closure of tonsillar pillars;
- Modified UPPP: additional mucosa and submucosal adipose tissue are removed superior and lateral to the tonsillar fossa and from the posterior soft palate;
- Laser assisted UPPP: outpatient procedure using laser incisions to shorten uvula and tighten soft palatal tissues; and
- Soft palatal implants: a less invasive procedure in which Dacron rods are inserted into the soft palate under local anesthesia (Sleep. 2010;33:1396-1407).
Complexities of AHI
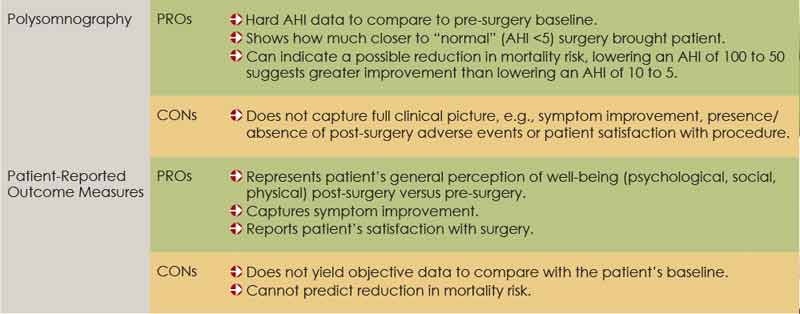
Determining OSA surgical success is complex at best. Many physicians believe that the efficacy of the procedure is best evaluated by monitoring the patient after surgery overnight in a sleep lab. This method yields hard data: The post-procedure AHI can be compared side by side with the person’s baseline. The challenge here again is patient compliance. While some patients are eager to discover just how much their condition has objectively improved, many physicians find it difficult to convince patients to spend another night in the sleep lab. Patients who feel significantly better may be particularly eager to put the whole OSA experience behind them. In addition, not all insurance providers are willing to reimburse a procedure they consider a mere exercise.
Change in AHI is one measurement that is commonly used to evaluate the success of OSA surgery. The accepted definition of a positive outcome cites a 50 percent reduction in AHI versus pre-operative AHI, achieving an AHI of 20 or less or both, but these criteria do not capture the full burden of OSA (Sleep Med Rev. 2010;14:283-285). According to Edward Weaver, MD, MPH, associate professor in the department of otolaryngology/head and neck surgery at the University of Washington in Seattle, “The commonly used AHI success criteria are arbitrary, and they were not defined by associated improvements in clinical outcomes, including survival, cardiovascular disease, quality of life or symptoms.”
In other words, they do not reflect useful information in the real world of clinical practice. Dr. Weaver explained, “There is no radical difference between a 51 percent and a 49 percent reduction in AHI; yet, according to convention, the first denotes a successful surgery and the second a failure. Similarly, a reduction in AHI from 50 to 25 probably delivers more health benefits than lowering AHI from 6 to 3, but the guidelines equate both of these as successful 50 percent reductions.”
Increased cardiovascular morbidity and mortality is seen more in patients experiencing oxygen desaturation than in those suffering from arousals. The latter group is affected by significant quality of life issues, including fatigue, increased risk of poor job performance and compromised ability to operate a motor vehicle, but the data concerning cardiovascular risk is more robust in the oxygen desaturation population.
Jonathan Hobson, MD, a consultant ENT in Cheshire, England and author of a recent study published in The Laryngoscope, is a strong proponent of using polysomnographic data as a critical part of evaluating surgical success, because the change in AHI represents the improvement in mortality risk (2012;122:1878-1881). “We are fairly certain that mild OSA has few serious long-term health consequences. But we are also fairly certain that moderate to severe OSA is what makes a patient more at risk for hypertension, myocardial infarction and stroke.” When it comes to reducing mortality risk, any reduction in AHI is probably beneficial, because most cardiovascular morbidities are associated with severe OSA. Moving a severe case into the mild or moderate column may reduce the patient’s overall disease burden, said Dr. Hobson.
Therefore, the impact of AHI reduction would be more completly evaluated by taking the starting point into account. A patient with an AHI of 100 who undergoes surgery and has a post-procedure AHI of 51 will most likely enjoy a greater improvement in mortality risk despite failing to achieve generally accepted surgical success. The patient is still at an increased risk for dying, but not as much as before surgery. Conversely, a patient with an AHI of 20 that is reduced by surgery to 10 can claim a successful procedure, even though his actual mortality risk will probably not be measurably improved. Although the change is statistically significant, it is not clinically significant.
What the Evidence Says
One of the challenges that arises when trying to evaluate the success of OSA surgery is the absence of rigorously proven, Level 1 evidence (randomized, placebo-controlled, double-blind clinical trials). Obviously, these studies are not possible when evaluating the success of surgery, because the experience and anatomical evidence of the procedure cannot be concealed from physicians and patients. But there are other types of evidence that can, and should, be considered. Non-randomized and good cohort studies do exist (Level 2 evidence) and would be beneficial. Case studies comparing MMA to CPAP have been done, and the results have been generalizable across sleep centers. The results appear in objective measures, including AHI and oxyhemoglobin nadir, suggesting they are free from any patient bias. Careful review of existing literature can point to the advantages of surgical interventions.
If CPAP treatment is deemed successful only when AHI is reduced to within normal parameters of 5 or less, it can be argued that surgery can only be labeled successful when it accomplishes the same reduction. Numerous studies, including a landmark study by Becker and colleagues published in 2003, have demonstrated that when AHI is at 5 or below, compared with a 50 percent reduction of the AHI, there is significant effect on lowering blood pressure, and therefore a meaningful decrease in cardiovascular risk (Circulation. 2003;107:68-73). Duration of CPAP use is also a factor that should be considered. In the Becker study, the patients were treated for the full night of sleep, an average of seven hours. The CMS definition of adequate CPAP compliance is four hours of usage 70 percent of the nights. This means that a patient who sleeps seven hours a night could be considered compliant with therapy even though treatment is only being received for 40 percent of sleep time. Surgical treatment provides treatment for 100 percent of sleep time.
These data suggest that patients using CPAP, with its higher success threshold, are healthier than those who undergo surgery. However, in 2004, Dr. Weaver published a study comparing mortality outcomes of patients using CPAP to that of patients who had undergone UPPP surgery. Overall, UPPP patients had better survival rates than CPAP patients (Otolaryngol Head Neck Surg. 2004;130:659-665).
It should be noted that all patients who received a CPAP device were included in the study, and there are no data regarding whether they used it regularly or at all. Considering compliance issues with CPAP therapy, it is likely that a significant number of these patients did not use their CPAP adequately and were therefore incompletely treated or untreated. However, surgery patients with partial improvement in AHI status experienced this partial benefit every night. The data suggest that gaining a partial treatment effect every night reduces mortality risk better than sporadic treatment benefits or no treatment at all.
Quality of Life
In treating OSA, there are measures of success beyond clinical metrics. “Physicians also have to look at how the patient feels as a result of the surgery,” said Dr. Hobson. “Patients consider the surgery successful if their symptoms are improved, if they experience less fatigue, improved daytime functioning, happier partners who are not being kept awake by snoring and, importantly, if they have not had complications as a result of the surgery.” UPPP surgery carries a risk for post-procedure adverse events, including difficulty swallowing, taste and smell disturbances, globus sensation, voice changes, persistent dry throat and nasal reflux. These discomforts can make patients regret choosing surgery, and make some physicians cautious about recommending the option.
Symptom and quality of life measures for evaluating surgical success, such as patient-recorded outcome measures (PROM), can be useful for assessing treatment effects in both the clinical and research settings. Published patient outcome data from sleep centers that include PROM feedback is more complete than reports that focus strictly on AHI improvement to determine surgical success rates.
Given the lack of consensus concerning how to best evaluate the success of OSA surgery, along with the risk of lasting and uncomfortable side effects, some physicians question the benefit of recommending the procedure. But many still see value in surgery for cases where CPAP does not deliver a solution, and encourage a more panoramic evaluation process, taking into account improvement over baseline and patient satisfaction.
Leave a Reply