Four tips for setting up an adverse-event reporting program for the solo or small-group practitioner
Hospital-Based Safety Programs: Making Them Work
Four tips for improving safety programs in hospitals.

Medicare Physician Payment Cut Averted
A 27.4 percent Medicare cut was scheduled to begin Mar. 1.
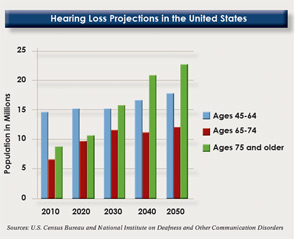
Otolaryngologists Concerned about Online Consumer Hearing Test
A subsidiary of UnitedHealth Group has launched an online hearing test and a line of lower-cost hearing devices that are generating alarm about patient safety among otolaryngologists.
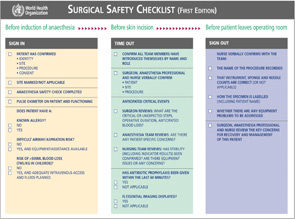
New Tool from the Joint Commission to Improve Surgical Consultations
Conflicting Evidence on Tobacco’s Effect on ESS Outcomes
Does smoking prevent sinus surgery from making patients feel better? Over the years, evidence and expert opinion have varied on this topic. As a result, some surgeons refuse to provide endoscopic sinus surgery (ESS) for active smokers, while others will operate because they believe surgery improves quality of life.

Review These Tips Before Leaving Your Medical Practice Job
Leaving a medical practice is never an easy decision. As you plan your exit strategy, be aware of these issues and address them proactively with your employer.

ICD-10 Implementation Delayed Indefinitely
Otolaryngologists may be wondering for a bit longer what their next step should be now that HHS has delayed the October 2013 implementation of the 10th revision of the International Statistical Classification of Diseases coding system (ICD-10).
There’s a (Medical) App for That
Five health care apps for mobile devices and tablets available to patients
Checklist Improves Communication During Patient Transfers
A standardized checklist and transfer protocol can reduce errors during patient handoffs following surgical or interventional procedures.
- « Previous Page
- 1
- …
- 251
- 252
- 253
- 254
- 255
- …
- 328
- Next Page »