
© Tyler Olson / shutterstock.com
Otologic complaints are commonly evaluated and treated in the emergency department (ED) setting. In a retrospective analysis of the Nationwide Emergency Department Sample (NEDS), among a weighted total of 388,904,009 ED visits in the years 2009 through 2011, 8,611,282 visits were attributed to a primary otologic diagnosis, representing 2.2% of all ED visits. Stratifying further by age, nearly 7% of all pediatric ED encounters involved otologic diagnoses (Laryngoscope. 2015;125:1926-1933).
The most common diagnoses among all age groups in the study included otitis media not otherwise specified (NOS) (60.6%), infected otitis externa NOS (11.8%), and otalgia NOS (6.8%). Other notable diagnoses included impacted cerumen (3.6%) and peripheral vertigo (0.9%). The most common diagnoses for pediatric patients were suppurative or unspecified otitis media (82.1%), followed by disorders of the external ear (9.0%) and other disorders of the ear (5.5%). In contrast, the most common diagnoses for adult patients were more evenly distributed, with suppurative or unspecified otitis media (32.4%) being the most common, followed by disorders of the external ear (28.8%), vertiginous syndromes (19.1%), and other disorders of the ear (12.3%).
Of otologic diagnoses resulting in hospital admission, the most common diagnoses were related to dizziness and vertigo, including benign paroxysmal vertigo (33.3%), labyrinthitis (12.1%), and vestibular neuronitis (8.1%).
Based on these analyses, Elliott D. Kozin, MD, clinical fellow in otolaryngology at the Massachusetts Eye and Ear Infirmary/Harvard Medical School in Boston, said that despite the fact that otologic complaints are commonly treated in the ED, there is a possibility that some otologic conditions are being underdiagnosed and undertreated. For example, one emergent complaint—sudden sensorineural hearing loss—was infrequently diagnosed in their study. “Estimates of sudden hearing loss are typically much higher based on reports in the literature, suggesting that ED providers may be missing opportunities to intervene in true otologic emergencies,” he added.
True Medical Emergencies
Very few ED visits for otologic complaints are actually warranted, said Sujana S. Chandrasekhar, MD, clinical professor at Hofstra-Northwell School of Medicine in Hempstead, N.Y., and president of the American Academy of Otolaryngology–Head and Neck Surgery Foundation (AAO-HNSF). In another study conducted by Massachusetts Eye and Ear Infirmary that focused on the subspecialty emergency room as an alternative model for otolaryngologic care, 6% of visits were for hearing loss (Am J Otolaryngol. 2014:35:758-765). “But hearing loss is not well evaluated in the ED, because no audiologic facility exists there, and, typically, not even a tuning fork is available,” said Dr. Chandrasekhar.
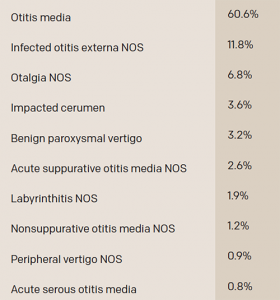
Most Common Otologic Diagnoses Made in the ED among All Patients with a Primary Otologic Complaint (2009-2011)
NOS, not otherwise specified
Source: Laryngoscope. 2015;125:1926-1933
Torree McGowan, MD, an emergency medicine physician at David Grant Medical Center in Fairfield, Calif., also said that it is rare for an ED patient with an ear complaint to have a true emergency. But mastoiditis and perichondritis, although uncommon, both present with ear pain and are justified emergencies. Lacerations involving the pinna are also injuries that must be repaired in a timely manner, to prevent deformity of the pinna caused by improper blood supply during healing. Auricular hematomas can create deformation of the pinna if not drained and dressed properly. Tinnitus can be caused by life-threatening conditions such as aspirin toxicity, carotid artery dissection or aneurysm, and anemia. Foreign bodies in the ear are usually fairly benign, unless they are button batteries, which can cause necrosis of the ear canal if not removed quickly.
Fever of unknown origin in a child younger than two years of age that originates in otitis media can result in meningitis, another true emergency, Dr. Chandrasekhar added.
Why Non-Urgent Patients Frequent the ED
Most patients with ear complaints are quickly evaluated and treated in EDs. “Multiple studies have shown that ED crowding, which is problematic at many hospitals nationwide, is affected by boarding admitted patients,” said Dr. Chandrasekhar. “Non-admitted patients with minor complaints actually have little impact on ED waiting times. However, on busy days, patients who present with ear complaints will likely be triaged to a lower triage category, because it’s rare that ear pain is life threatening. These patients may have prolonged waits for evaluation because other patients with potentially more life-threatening conditions are evaluated first.”

© sumroeng chinnapan / shutterstock.com
According to a report from the Centers for Disease Control, “Emergency Room Use among Adults Aged 18–64, January–June 2011,” the top reasons patients cited for going to an ED included lack of access to other providers (79.7%); seriousness of the medical problem (66%); only a hospital could help (54.5%); the doctor’s office wasn’t open (48%); and the problem was too serious for a doctor’s office (42.5%) (report available at cdc.gov).
“Business hours only account for 27% of a week’s hours,” Dr. McGowan said. “For the remaining 73% of the time, EDs are often the only places open when patients are in pain or are concerned about their health. Further, we are forbidden by The Emergency Medical Treatment and Labor Act (EMTALA) to require payment prior to evaluation, so we are often the medical care of last resort for patients who are uninsured or underinsured.”
Dr. McGowan also noted that we live in a society that is often unwilling to wait for results, and EDs have a streamlined system to obtain diagnostic studies. “Patients may have to wait to be seen, but they don’t have to wait weeks for an appointment or to get an imaging study or laboratory result,” she said.
Hearing loss is not well-evaluated in the ED, because no audiologic facility exists there and, typically, not even a tuning fork is available. —Sujana S. Chandrasekhar, MD
Reducing Non-Urgent Visits
Despite overcrowding and non-emergent visits, emergency physicians wouldn’t want to discourage patients from coming to the ED. “The American College of Emergency Physicians states that if a prudent layperson could reasonably be concerned that an emergency exists, they deserve the right to be seen in the ED and have that visit covered by their health insurance as an emergency department visit,” Dr. McGowan said.
That being said, “Increased access to primary care after hours and on weekends decreases the number of patients seeking care in the ED,” Dr. McGowan said. “While urgent care centers can be a great option, they are staffed with physicians from various backgrounds, and many are not trained in emergency medicine.”
Dr. Chandrasekhar believes that educating primary care providers as well as patients on what constitutes a true otolaryngology emergency could help lower the number of non-urgent visits to the ED. The AAO-HNSF does this by including ED representation on pertinent clinical practice guidelines (CPGs). “Of 16 CPGs in publication or in development at the AAO-HNSF, four (i.e., sudden hearing loss, Bell’s palsy, benign paroxysmal positional vertigo, and evaluation of the neck mass in adults) have an emergency physician on the guideline development group (GDG),” she reports. “Every member of the GDG has an equal voice and equal writing responsibilities for each CPG.”
The AAO-HNSF also partners with the American Board of Internal Medicine Foundation to participate in its Choosing Wisely campaign, which promotes conversations among clinicians and patients by helping patients choose care that is supported by evidence, not duplicative of other tests or procedures already received, free from harm, and truly necessary. “This helps them to be able to fully participate in their healthcare decisions,” Dr. Chandrasekhar said.
Despite the low number of patients using the ED for true otologic emergencies, emergency physicians feel that it is their duty to accommodate all patients. While there are ways to deter ED visits, such as education and increasing access to primary care, some emergent cases do indeed exist.
Karen Appold is a freelance medical writer based in Pennsylvania.
Key Points
- Despite the fact that otologic complaints are commonly treated in the ED, there is a possibility that some otologic conditions are being underdiagnosed and undertreated.
- Very few ED visits for otologic complaints are actually “true” medical emergencies.
- Educating primary care providers as well as patients on what constitutes a true otolaryngology emergency could help lower the number of non-urgent visits to the ED.
Are Specialty Emergency Departments a Viable Solution for Overburdened ERs?
The Institute of Medicine Committee on the Future of Emergency Care has recommended developing a system of emergency care to increase access to specialty care. “Historically, there used to be more dedicated otolaryngologic emergency rooms,” said Elliott D. Kozin, MD, clinical fellow in otolaryngology at the Massachusetts Eye and Ear Infirmary (MEEI)/Harvard Medical School in Boston. “Today, the MEEI has one of the last remaining 24/7 emergency rooms that focuses on otolaryngology and ophthalmology-related complaints. The MEEI emergency room is a unique healthcare provider model that provides direct access to specialists in the acute setting.”
In a study led by clinical fellows at the MEEI aimed at characterizing practice patterns in a dedicated otolaryngology emergency department (ED), researchers concluded that, “While all otolaryngologic complaints often do not require specialist-level care, a regionalized system of expertise, whether a stand-alone ED or a dedicated team focused on otolaryngologic complaints by emergency room and/or otolaryngology providers, may lead to improved care coordination and address many of the concerns previously introduced. Moreover, as the implementation of the Patient Protection and Affordable Care Act nears completion, the anticipated number of common otolaryngologic complaints seen in EDs will likely increase significantly.” (Am J Otolaryngol. 2014:35:758-765)
Otolaryngologists should be actively involved in acute care policy decisions and developing emergency department treatment algorithms.
Of 12,234 patient visits at the MEEI ED between January 2011 and September 2013, 50% of patients came in for auditory and vestibular problems and 92.3% of patients were discharged after their ED visit.
Because many otolaryngologic complaints, such as hearing loss and dizziness, are commonly evaluated in the ED setting, Dr. Kozin said that, at minimum, otolaryngologists should be actively involved in acute care policy decisions and in the development of ED treatment algorithms.
Possible Drawbacks
While weighing in on the feasibility of having an ED dedicated to otolaryngologic complaints, some physicians also see downsides to this model. “One of the major drawbacks of a specialty-specific ED is that ED patients present as undifferentiated patients,” said Torree McGowan, MD, an emergency medicine physician at David Grant Medical Center in Fairfield, Calif. “Emergency physicians are unique in that they consider all systems and specialties in their evaluation, and then narrow the differential diagnosis to the right specialist,” she added. “We evaluate an undifferentiated patient based on their chief complaint, rather than managing a known disease—which is how most specialists operate.”
Michael Sore, MD, clinical director of the Largo Medical Center Department of Emergency Medicine in Largo, Fla., also thinks that specialty-specific EDs are not the right answer. “I have had several cases where a patient presented with a seemingly straightforward otologic complaint that turned out to be a life-threatening condition that required assistance from specialists other than an ENT,” he said. “One case was a patient who complained of left ear pain that turned out to be an acute ST segment elevation myocardial infarction. In another case, the patient complained of a severe, left-sided sore throat which was diagnosed as a carotid artery aneurysm.”
J. Thomas Roland, Jr., MD, Mendik Foundation Professor of Otolaryngology, chair of the department of otolaryngology-head and neck surgery, and professor in the departments of otolaryngology and neurosurgery at NYU Langone Medical Center in New York City, doubts that a facility dedicated to otolaryngologic care would be used that often, as data has shown that not many patients visit the ED for such issues. But if it offered 24-hour care for all problems related to the ear, nose, and throat, it might be frequented fairly often—especially after typical physician’s hours. “Patients would have immediate access to specialists for their needs,” he said. “But it could make a financial impact on the ENT community, which makes a significant part of their living by caring for emergent ENT problems.”—KA