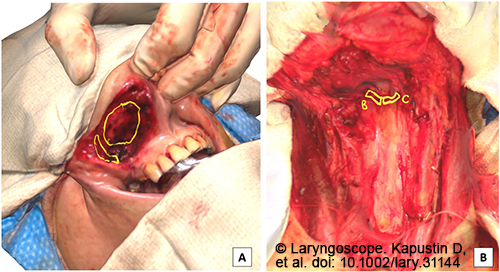
Figure 2. Two examples of defect annotations. (Left) Upper lip resection with annotations of supplemental margins harvested including deep lateral margin and subcutaneous margin. (Right) Laryngopharyngectomy defect with annotations demonstrating supplemental right and left superior submucosa of the posterior pharyngeal wall.
At the same time as the 3D defect model was being annotated intraoperatively by the surgeon, the pathologist in the frozen section laboratory appropriately annotated the resection specimen model to reflect margins at-risk (Fig. 2). The results of the margin analysis were communicated to the surgeon in the operating room. Supplemental margins were indicated on the defect scan only when supplemental margins were required based on analysis of the main specimen.
Explore This Issue
December 2023A Zoom video conference was conducted between the operating room and frozen section laboratory, during which the annotated models were shown and discussed. The surgeon oriented the pathologist as to the location and breadth of supplemental tissue harvested. After the Zoom conference, still images of the annotated models were captured, deidentified, and saved into the secure Mount Sinai network.
RESULTS
Ten 3D surgical defect models were annotated using Procreate (Fig. 1) during 10 consecutive head and neck oncologic resections. Transferring the completed scan from the EXScan companion software into Procreate took five minutes and 26 seconds when averaged across 10 trials (SD = 1 minute, 15 seconds). The duration of annotation itself by the surgeon and pathologist was negligible, typically lasting less than 30 seconds in duration.
By using Procreate on an iPad, the surgeon could annotate intraoperatively without breaking scrub to indicate the breadth of supplemental margins harvested in real time. Additionally, the pathologists could manipulate and annotate the virtual 3D model seamlessly using the iPad to demonstrate margins at-risk. Finally, virtually orienting the pathologist to the harvested margins by video conference eliminated the surgeon’s transition time scrubbing in/out and eliminated the risk of requiring additional tissue samples due to miscommunication between surgeon and pathologist. A video demonstration is included.