Explore This Issue
October 2018Comment: There remain several theories that attempt to explain how cholesteatomas develop. All of these have inconsistencies that weaken them. The most recent theory—the mucosal traction theory—is carefully examined by these authors, who ultimately show that, like the others, this theory is flawed. —Andres Bur, MD
What is the distribution of ciliated epithelium in the human middle ear and its potential role in the formation of cholesteatoma?
Bottom line
The paucity of ciliated epithelial cells on the medial side of the tympanic membrane and the lateral surface of the ossicles in the epitympanum in cases with cholesteatoma and/or chronic otitis media does not support the mucosal migration theory of cholesteatoma formation.
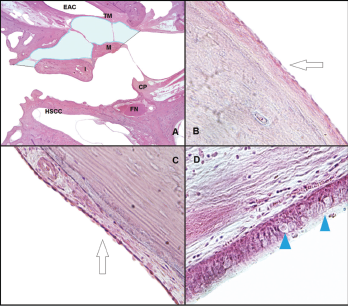
Histological analysis of the middle ear space. (A) Slide from a left ear, at the level of the pars flaccida, showing the space where the ciliated cells were counted at the epitympanum: lateral side of the malleus and incus, and medial side of the lateral wall. The light blue area represents the area where the ciliated cells were counted (H&E, 1 × magnification). (B) The arrow shows the flat epithelium located at the lateral side of the malleus (H&E, 10 × magnification). (C) The arrow shows the flat epithelium located at the medial side of the lateral wall at the epitympanum (H&E, 10 × magnification). (D) Histological view of the respiratory-like epithelium that covers the lateral wall of the protympanum toward the Eustachian tube. The arrowheads show the goblet cells located at this space (H&E, 40 × magnification). CP = cochleariform process; EAC = external auditory canal; FN = facial nerve; H&E = hematoxylin and eosin; HSCC = horizontal semicircular canal; I = incus; M = malleus; TM = tympanic membrane.
Credit: © 2018 The American Laryngological, Rhinological and Otological Society, Inc.
Background: A cholesteatoma is a non-neoplastic epithelial lesion that contains layers of keratin in a cavity lined by keratinizing squamous epithelium and subepithelial connective tissue. Although benign, it can cause serious complications by eroding nearby structures or precipitating infection. Surgical removal of the lesion is considered the only effective medical therapy. There are several theories on the etiopathogenesis of acquired cholesteatoma, including one based on the premise that a squamous pouch is drawn inward by traction exerted by the interaction of opposing ciliated epithelial surfaces of middle ear mucosa on the medial surface of the tympanic membrane and the lateral surface of the ossicles.
Study design: Comparative study of 73 human temporal bones.
Setting: Otopathology Laboratory in the Department of Otolaryngology, University of Minnesota, Minneapolis.
Synopsis: The temporal bones were separated into five groups: 1. cholesteatoma; 2. chronic otitis media without cholesteatoma (COM); 3. retraction pockets (RPs); 4. cystic fibrosis (CF); and 5. a control group with no middle ear disease. In the epitympanum: There were no differences in the number or distribution of ciliated cells between the pars tensa and pars flaccida of the tympanic membrane among the groups. The mean number of ciliated cells at the lateral epitympanum’s mucosal lining and the malleus and incus’s lateral surface were significantly reduced in bones with cholesteatoma.
There were fewer ciliated cells in the RP group compared with non-diseased ears; when present, they were usually located at the lateral wall of the epitympanum, not on the ossicles. In the tympanic membrane: The mean number of ciliated cells was decreased in the cholesteatoma compared to RP groups. In the protympanum: Ciliated cells were plentiful for all four conditions studied.
The mean number of ciliated cells in the lateral wall of the protympanic space was decreased in the group with cholesteatoma and COM compared to RP, CF, and control groups. Some ciliated cells were found at the tympanic membrane’s anterior annulus and at the posterior portion of the handle of the malleus, in contact with the tympanic membrane. The epithelium covering the ossicles’ lateral face at the epitympanum and at the medial surface of the tympanic membrane consisted of flat simple squamous epithelium.
Citation: Pauna HF, Monsanto RC, Schachern P, et al. Evidence against the mucosal traction theory in cholesteatoma. Laryngoscope. 2018;128:1663–1667.