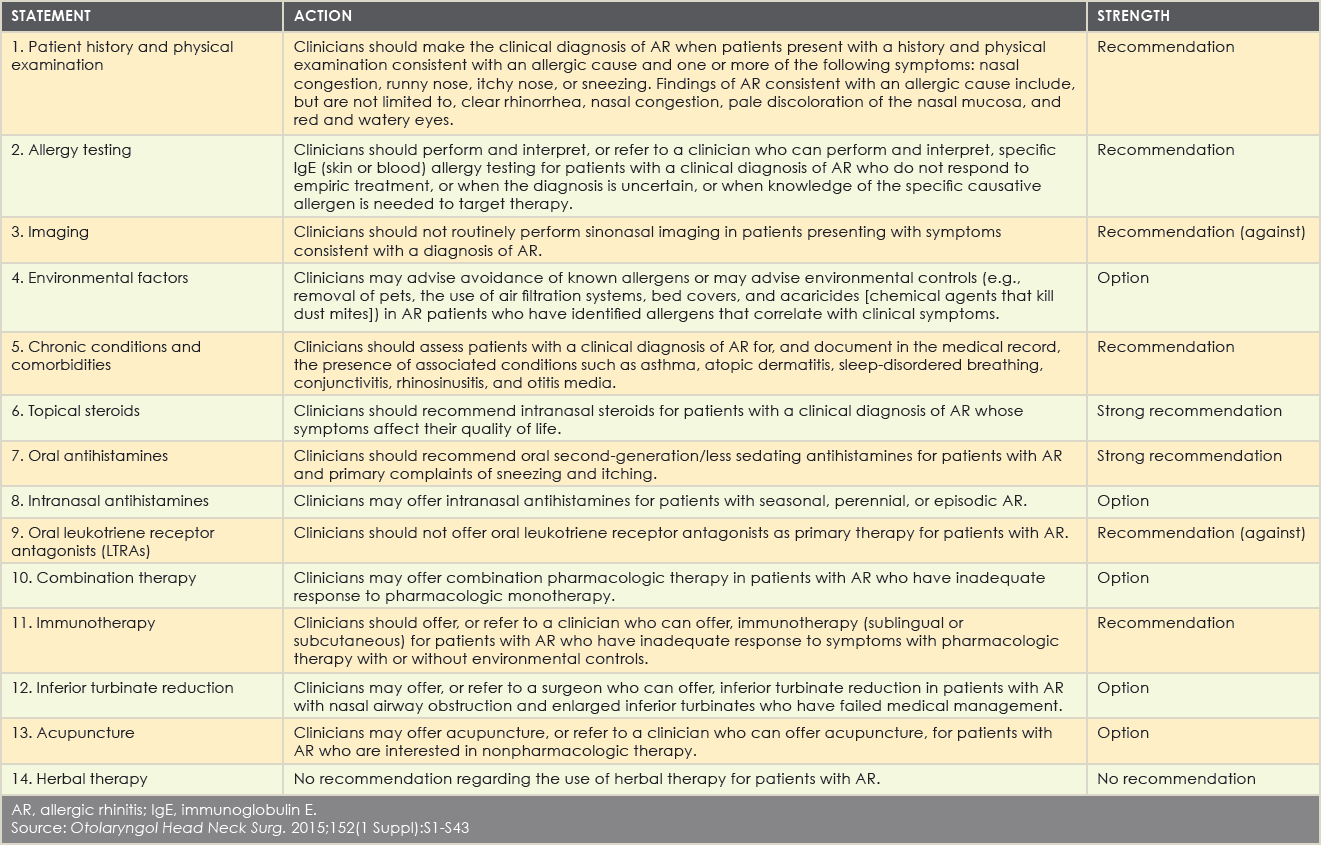
The guideline also advises clinicians to recommend oral second-generation/less sedating antihistamines for patients with AR whose primary complaints are sneezing and itching. “There is a knowledge gap in that most patients recognize Benadryl as the go-to antihistamine,” Dr. Mims said. “Instead, practitioners should promote the use of effective symptom-directed therapy.” According to the guideline, while oral antihistamines may not be as effective as intranasal steroids, they are adequate for many patients with mild to moderate disease and have the advantage of lower cost, rapid onset of action, and effectiveness for intermittent symptoms.
Explore This Issue
April 2015The guideline also supports the use of topical intranasal steroids for patients with a clinical diagnosis of AR whose symptoms affect their quality of life. “These medications have shown clear benefits in randomized controlled trials,” Dr. Wise said. “However, frequently patients say that a nasal steroid was ineffective. After digging deeper, we learn that the patient was not educated on its proper use. Many patients assume that nasal steroids work quickly, like topical intranasal decongestants, with symptomatic benefit in minutes. But many of these medications take hours or days to reach appropriate efficacy.”
In addition, the guideline directs clinicians toward certain combinations of pharmacologic therapy that are more effective than other combinations. “One of the common combinations of medications is an oral antihistamine and a topical nasal steroid spray, but studies haven’t shown that there is much additional benefit in taking them in combination compared to taking a nasal steroid spray alone,” Dr. Mims said. “The guideline also explains why changing to another kind of allergy medication might be a better recommendation than multiple medications in some patients.”
When medical therapy and counseling don’t effectively control symptoms, the guideline recommends referring patients to specialists for possible further testing and treatment. “This may involve a higher level of expert advice on how to best use pharmacological agents or the possible use of allergy testing and immunotherapy, which have been very effective in this population,” Dr. Mims said.
Summary of Guidance Action Statements
(click for larger image)
AR, allergic rhinitis; IgE, immunoglobulin E.
Source: Otolaryngol Head Neck Surg. 2015;152(1 Suppl):S1-S43
Immunotherapy
The guidelines advise clinicians to refer patients with AR who have an inadequate response to pharmacologic therapy with or without environmental controls to a clinician who can offer immunotherapy—either sublingual or subcutaneous. The guideline is the first to discuss sublingual tablets since the FDA approved them in 2014.