Does use of narrow band imaging (NBI) influence observer agreement while making diagnostic decisions using rigid endoscopy of the upper aerodigestive tract?
Bottom Line
The addition of NBI to conventional white light imaging (WLI) improves inter- and intraobserver agreement for diagnosing (pre)malignant lesions in the larynx, hypopharynx, and oropharynx and therefore improves the reliability of endoscopic examinations.
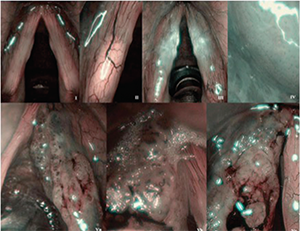
Examples of different Ni classification types applied in studied group of patients. Type I: thin, interconnected vessels. Type II: enlarged vessel diameter. Type III: vascular patterns obscured by white mist. Type IV: small regularly distributed dots. Type Va: solid or hollow thick brown spots with various shapes. Type Vb: destroyed loop, its remnants are visible as line-like shapes. Type Vc: combination of type Va and Vb, irregular distribution.
Background: NBI is a relatively new endoscopic technique for detecting (pre)malignant lesions in the head and neck area, and is based on the principle that the wavelength of light influences the penetration depth in tissues: The larger the wavelength, the deeper the penetration. Currently, Ni’s intraepithelial papillary capillary loop (also called intrapapillary capillary loop) classification is most frequently used to classify mucosal laryngeal lesions. NBI increases the contrast between a lesion and healthy epithelium, and seems to be a promising technique for differentiation between benign and (pre)malignant lesions.
Study design: Retrospective study.
Setting: Department of Otorhinolaryngology/Head and Neck Surgery, University Medical Center Groningen, Netherlands.
Synopsis: There have been no previous studies on inter- and intraobserver reliability for use of NBI in the upper aerodigestive tract. The purpose of this study was to evaluate observer agreement performing three subgroup analyses: assessment of a lesion’s nature (benign vs. malignant), consistency in application of the Ni classification, and evaluation of the presence of brown dots. Because previous studies suggested that NBI was particularly useful for inexperienced observers, the authors evaluated three different observer groups based on level of experience.
A total of 100 routinely collected pictures of laryngeal, hypopharyngeal, and oropharyngeal lesions were used. Rigid endoscopies and patient data collection were performed according to standard protocol. Twelve observers, grouped in different levels of experience, assessed all lesions twice with a two to four week interval. Fleiss and Cohen’s kappa (k) values were calculated to assess inter- and intraobserver agreement. Overall interobserver agreement increased from ĸ = 0.34 to ĸ = 0.40 by adding NBI to WLI (WLI and WLI plus NBI, respectively). In experienced observers, an improvement from ĸ = 0.39 to ĸ = 0.43 was observed; in less-experienced observers an improvement from ĸ = 0.30 to ĸ = 0.37 was observed. Overall intraobserver agreement increased from moderate (ĸ = 0.54) to substantial (ĸ = 0.63) with addition of NBI. Intraobserver agreement for less-experienced observers improved remarkably when WLI was combined with NBI (ĸ = 0.51 vs. ĸ = 0.67).
Citation: Zwankenberg Manon A. Dikkers FG, Wedman J, et al. Narrow band imaging improves observer reliability in evaluation of upper aerodigestive tract lesions. Laryngoscope. 2016;126:2276–2281.