 TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope article, visit Laryngoscope.
TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope article, visit Laryngoscope.
Explore This Issue
October 2021BACKGROUND
Non-melanoma skin cancer (NMSC) is the most prevalent type of malignancy worldwide, with more than 1 million cases of NMSC diagnosed in the United States each year. The most common types of NMSC are basal cell carcinoma (BCC) and cutaneous squamous cell carcinoma (cSCC). Numerous risk factors exist for NMSC, including ultraviolet radiation, ionizing radiation, genetic disorders, chronic inflammation, and immunosuppression.
Compared with the general population, patients who are chronically immunosuppressed have a significantly increased risk of developing NMSC; organ transplant recipients are 65 to 250 times more likely to develop cSCC and 10 to 16 times more likely to develop BCC. In immunosuppressed patients, prevention strategies, frequent surveillance, and early intervention are critical for reducing the morbidity and mortality associated with NMSC.
When treating patients with NMSC, it is important to determine if they are at low risk or high risk for recurrence, as this has important prognostic implications and affects their recommended treatment algorithm. Several characteristics including lesion size, location, borders, histopathologic features, and patient history of prior radiation therapy or immunocompromised state factor into the determination of whether a patient is at low risk or high risk. Based on the 2021 National Comprehensive Cancer Network guidelines (see Figure 1), all patients who are immunosuppressed should be classified as having high-risk lesions.
BEST PRACTICE
Several factors, such as tumor size, location, and histopathological features, must be considered when deciding on surgical margins for NMSC. For low-risk cSCC, 4 to 6 mm margins are recommended, whereas for low-risk BCC, the recommendation is for 4 mm margins. Per the NCCN guidelines, chronic immunosuppression places patients with cSCC and BCC into the high-risk category. For patients with high-risk cSCC and BCC, the standard of care is complete circumferential peripheral and deep margin assessment; however, if this is not possible, then standard surgical excision with 4 to 6 mm and 4 mm margins, respectively, is recommended
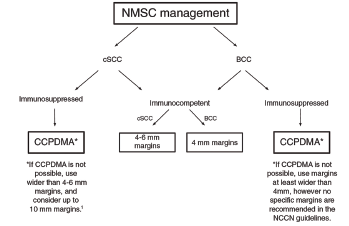
Figure 1. Management of NMSC based on the National Comprehensive Cancer Network guidelines. BCC = basal cell carcinoma; CCPDMA = complete circumferential peripheral and deep margin assessment; cSCC = cutaneous squamous cell carcinoma; NMSC = nonmelanoma skin cancer.