Explore This Issue
August 2012

Management:
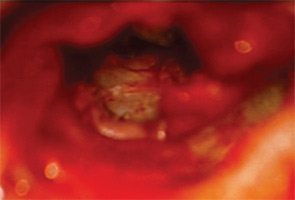
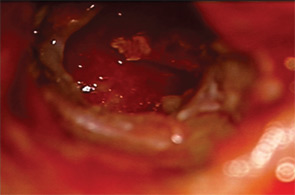
The patient underwent a middle ear exploration. To maximize exposure, a post-auricular approach was utilized. The tympanic membrane perforation seen previously in the clinic was nearly healed, despite the presence of a middle ear foreign body. Blue foam material completely filled the middle ear, including hypotympanum, mesotympanum and epitympanum. The foreign body completely encased the ossicles (Figure 1). A decision was made to use a flexible CO2 laser (Omniguide), along with a #1 knife, to break the amorphous material into manageable fragments that could be more easily dissected. Meticulous dissection was performed around the ossicles to preserve ossicular continuity. The foreign body was completely removed in a piecemeal fashion using cupped forceps. A tragal cartilage graft, together with a previously obtained temporoparietal fascial graft, was used for tympanic membrane reconstruction.
Discussion:
Certain foreign bodies in the ear can involve the middle ear, making removal difficult. A few sporadic reports describing middle ear foreign bodies as a complication of hearing aid ear mold fitting have been described.1-4 Proper fitting of hearing aids follows established guidelines and rarely results in serious complications.1 One important step to ear mold fitting is placement of a well-positioned and well-sealed protective otoblock and atraumatic injection of properly prepared ear mold material.5,6 Ear mold material escaping beyond the otoblock barrier can occur in cases of uncooperative patients, improper placement of the otoblock or overly aggressive injection of the ear mold material.
One author described molding material that entered a patient’s middle ear through pre-existing tympanic membrane perforations in both ears.7 Another report noted that all patients in their series with ear mold complications had pre-existing abnormalities in their aural anatomy, including tympanic membrane perforations, retraction pockets and mastoidectomy cavities, suggesting that patients with altered aural anatomy are at particular risk.8
Various techniques have been described for the removal of retained foreign body debris, including routine tympanomastoidectomy. In canal-wall-down patients with residual ear mold fragments after mold fitting, revision meatoplasty has been reported.1
One author recommends that the stapes be directly visualized and the incudostapedial joint separated during removal of mold material that has encased the ossicles.8 We described a novel otologic method for removal not previously described in the literature using a combination of CO2 laser and cold knife dissection, while keeping the ossicles in continuity and preventing avulsion.
Mastoidectomy was not warranted in our particular case, because the entire mold could be removed piecemeal through the canal using the combination of the CO2 laser and cold knife dissection. In certain cases, however, a mastoidectomy may be beneficial to gain access to the epitympanum for retained FB fragments. The integrity of the ossicular chain was maintained in part due to the patient presenting to our clinic promptly after the incident, allowing a timely operative intervention. Reports demonstrate erosion of ossicles and ossicular discontinuity after delayed diagnosis.1,8
Soon after his surgery, our patient was seen and reported hearing improvement and pain resolution. At four months post surgery, the patient was well healed, and his hearing had improved. His audiogram showed near complete closure of air bone gap and resolution of TM perforation.
References
- Kohan D, Sorin A, Marra S, et al. Surgical management of complications after hearing aid fitting. Laryngoscope. 2004;114(2):317-322.
- Hof Jr, Kremer B, Manni JJ. Mould constituents in the middle ear, a hearing-aid complication. J Laryngol Otol. 2000;114(1):50-52.
- Schimanski G. Silicone foreign body in the middle ear caused by auditory canal impression in hearing aid fitting [in German]. HNO. 1992;40(2):67-68.
- Syms CA III, Nelson RA. Impression-material foreign bodies of the middle ear and external audiotry canal. Otolaryngol Head Neck Surg. 1998;119(4):406-407.
- Kohan D, Levy L. Aural Rehabilitation Hearing Aids and Assistive Listening Devices. Alexandria, Va.: SIPAC American Academy of Otolaryngology-Head and Neck Surgery; 1999.
- Goldenberg RA. Hearing Aids: A Manual For Clinicians. Philadelphia: Lippincott Williams and Wilkins; 1996.
- Kadish H. Ear and nose foreign bodies: “It is all about the tools.” Clin Pediatr (Phila). 2005;44(8):665-670.
- Jacob A, Morris TJ, Welling DB. Leaving a lasting impression: ear mold impressions as middle ear foreign bodies. Ann Otol Rhinol Laryngol. 2006;115(12):912-916.
Leave a Reply