Results have been found to be good for mild to moderate sleep apnea, with more sessions translating to greater success. But patients still showed residual apnea (Otolaryngol Head Neck Surg. 2003;128:848-861). Tongue-channeling, which is not heat-based and is performed over one or two sessions, involves the shrinkage of deep musculature and connective tissue. Large reductions in AHI and sleepiness have been seen in a case series with this approach (J Clin Sleep Med. 2013;9:117-124). “It’s typically, in my mind, an adjunctive treatment,” Dr. Weaver said.
Explore This Issue
November 2016“I use radiofrequency [tongue reduction] for patients who have primary complaint of snoring and very mild sleep apnea,” said panel moderator Michael Friedman, MD, professor of otolaryngology-head and neck surgery at Rush University Medical Center in Chicago and medical director for Chicago ENT.
TORS for Tongue Reduction
Erica Thaler, MD, professor of otolaryngology-head and neck surgery at the University of Pennsylvania in Philadelphia, said she started using transoral robotic surgery (TORS) for base of tongue reduction a few years ago. “It has evolved to be my way of most often dealing with challenging tissue at the base of the tongue and dealing with hypopharyngeal obstruction,” she said. Her outcome data show that, among patients who had undergone no prior surgery, AHI was reduced by 67%.
We want to make the most accurate determination of the anatomical issues and treat patients individually. —Eric Kezirian, MD, MPH
Dr. Thaler said that she has no hard cap on body mass index for TORS candidates and added that a patient’s physiognomy is an important consideration: If a patient has more body mass below the neck, he or she could be a candidate despite having a high BMI, and vice versa. “It’s not a trivial procedure of getting the patient through postoperative pain management,” she said. “It’s probably the toughest part of this for me, but it’s great surgery to handle this area.”
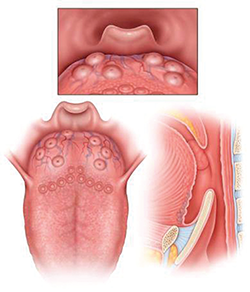
LTH Grade 1: Lymphoid tissue scattered over tongue, does not cover entire surface of tongue base.
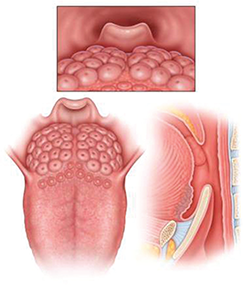
LTH Grade 2: Lymphoid tissue covering entire tongue base, limited vertical thickness.
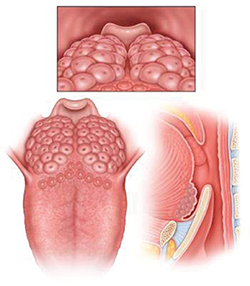
LTH Grade 3: Lymphoid tissue covering entire tongue base, vertical thickness between 5-10 mm, approximately 25-75% of height of epiglottis.
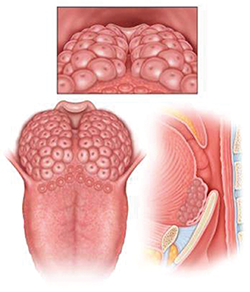
LTH Grade 4: Lymphoid tissue covering entire tongue base, vertical thickness approximately 1 cm, rises above tip of epiglottis.
Rating Lingual Tonsillar Hypertrophy
Dr. Friedman introduced a new way of systematically rating the degree of lingual tonsillar hypertrophy (see figure above):
- Grade 1: Lymphoid tissue scattered over the tongue;
- Grade 2: Lymphoid tissue covering the tongue but with limited vertical thickness;
- Grade 3: Between 25% and 75% of the height of the epiglottis; and
- Grade 4: Vertical thickness rising above the tip of the epiglottis.
“If we are going to study the efficacy of lingual tonsillectomy, we have to have a common language,” he said. “We can’t have one study doing Grade 4 tonsils and one study doing Grade 1.”
Endoscopic Coblation Open Tongue Base Resection
Hsin-Ching Lin, MD, associate professor of otolaryngology at Chang Gung University and vice chair of otolaryngology at Kaohsiung Chang Gung Memorial Hospital in Kaohsiung, Taiwan, described his center’s success with endoscopic coblation open tongue base resection, a procedure geared toward those who have moderate-to-severe OSA, have a large base of tongue on exam, and have failed continuous positive airway pressure (CPAP) treatment.