INTRODUCTION
Drug-induced sleep endoscopy (DISE) as a means of upper airway diagnostics was first introduced by Croft and Pringle in 1991 with the use of midazolam sedation (Clin Otolaryngol Allied Sci. 1991;16:504-509). Since then, there have been a variety of medications and techniques introduced to modify and improve the ability to evaluate sites of upper airway collapse in a drug-induced “sleep” state. However, our current methods of DISE provide only a qualitative visualization of upper airway collapse and do not provide any quantitative information regarding the degree or severity of upper airway collapsibility.
Explore This Issue
October 2022The use of continuous positive airway pressure (CPAP) during drug-induced sleep endoscopy has been previously described as a diagnostic tool to assess upper airway collapse. Civelek and colleagues performed a double-blind study of 16 patients and reported that CPAP titration pressures during sleep endoscopy under propofol sedation approximated pressures obtained during an in-laboratory titration within natural sleep (Laryngoscope. 2012;122:691-695). In 2019, Lee and colleagues demonstrated that a preoperative therapeutic positive airway pressure (PAP) level less than 8 cm H2O had a 92% positive predictive value for surgical success in hypoglossal nerve stimulator implantation (HGNS) as compared to only 44% in patients with PAP levels greater than or equal to 8 cm H2O (J Clin Sleep Med. 2019;15:1165-1172). A follow-up study by the same group used therapeutic nasal PAP during DISE to examine the palatal opening pressure of the airway (POP). They noted that a POP level less than 8 cm H2O correlated with a positive predictive value of 82.4% surgical success for HGNS as defined by a 50% reduction in the apnea-hypopnea index (JAMA Otolaryngol Head Neck Surg. 2020;146:691-698). Dedhia and colleagues recently published their updated DISE-CAD protocol (drug-induced sleep endoscopy-characterization of airway dynamics) in which they extracted relevant anatomic and physiologic parameters of each patient’s upper airway during sleep endoscopy (ORL J Otorhinolaryngol Relat Spec. 2021;1-6).
Multiple major academic centers across the country are currently evaluating the benefits of using PAP during DISE. While there appears to be an abundance of information that can be gleaned from determining the opening pressures of the airway—and sleep surgeons across the country are interested in implementing the protocol—it has previously been relegated primarily to research settings and has had limited practical application in the clinical setting due to barriers of cost and efficiency.
Herein, we describe a novel method to implement drug-induced sleep endoscopy with positive airway pressure (DISE-PAP) in a cost-effective and highly clinically efficient manner, allowing it to be immediately introduced in both clinical and research settings.
METHOD
DISE-PAP is utilized in patients >18 years of age with a diagnosis of obstructive sleep apnea who are intolerant of CPAP. In order to make DISE-PAP affordable in the clinical setting, supplies were purchased through the operating room, eliminating direct cost to the surgeon while also allowing for minimal increased patient billing.
The total cost of PAP supplies charged to patients for each DISE was $18.60. These fees were then bundled into the total hospital bill for the procedure. CPAP machines may be purchased online, and typically range between $300 and $1,500 depending upon make and model.
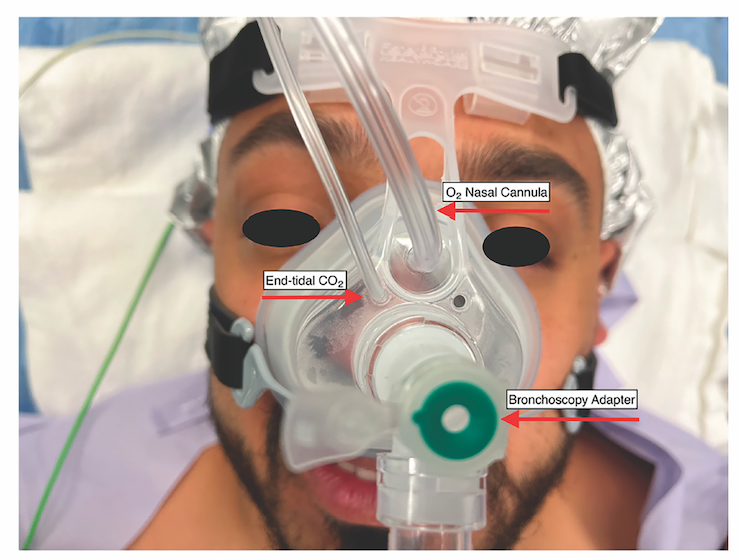
Figure 1. Mask set-up with placement of oxygen, end-tidal CO2, and bronchoscopy adapter.
DISE PAP Assembly. In order to maximize clinical efficiency, the equipment may be assembled preoperatively by operating room staff (see supporting video). The CPAP machine is programmed to deliver a 5-minute ramp from 4 to 20 cm H2O. The proximal end of the CPAP tubing is inserted into the CPAP machine, and the viral filter is inserted into the distal end of the tubing. The mask is then assembled by removing the plastic 90° elbow from the mask and inserting the bronchoscopy adapter in its place. The oxygen tubing is inserted into the CPAP mask by cutting the distal end of an oxygen nasal-cannula tubing and inserting it into the mask. The end-tidal CO2 tubing is cut at a 45° angle and inserted into one of the pressure-release valves of the mask (Figure 1).
Drug-Induced Sleep Endoscopy. After a procedural timeout is performed, a bolus of propofol is administered and a steady infusion rate of propofol is initiated. While the TCI technique has been shown to provide a larger window of steady-state sedation, this is not available at our institution so a steady infusion rate over time allowed for a more consistent state of sedation. The nasal mask is then placed over the patient’s nose (Figure 1). Once secure, the flexible fiberoptic nasopharyngoscope is passed through the bronchoscopy adapter and into the naris predetermined to be less obstructed by septal deviation or other deformity. Once the patient reaches the appropriate depth of sedation, a formal upper airway evaluation is executed. Once the evaluation is complete, the CPAP tubing is connected to the mask via the bronchoscopy adapter and the CPAP machine is turned on to utilize the preprogrammed 5-minute ramp from 4 to 20 cm H2O. The airway is visually examined until complete resolution of airway obstruction and snoring is observed at the level of the soft palate, which was deemed the palatal opening pressure (JAMA Otolaryngol Head Neck Surg. 2020;146:691-698). The pressure needed to resolve obstruction and snoring at the level of the lateral walls (lateral wall opening pressure, or LOP), tongue base opening pressure, and epiglottis opening pressure were also determined. The overall pressure needed to resolve complete upper airway obstruction and snoring was deemed the pharyngeal opening pressure (ORL J Otorhinolaryngol Relat Spec. 2021;1-6). Upon completion of the sleep endoscopy, the flexible nasopharyngoscope is removed from the patient’s naris. The mask is then removed and the patient is returned to anesthesia. The average procedure time was 12 to 15 minutes. DISE PAP added approximately 5 minutes per case.
RESULTS
Use of positive airway pressure during sleep endoscopy has shown increasing promise in improving patient selection for hypoglossal nerve stimulation, and has the potential for improving patient selection for other sleep apnea interventions (JAMA Otolaryngol Head Neck Surg. 2020;146:691-698). The current cost of equipment as well as preparation and assembly of the equipment has made DISE-PAP impractical for incorporation into common practice in high-volume clinical settings. Exploiting this novel protocol, we have managed to transform a procedure that previously cost hundreds of dollars per patient to $18.60 per patient. This protocol is both financially feasible and clinically efficient, allowing DISE-PAP to become a readily available tool for sleep surgeons.