INTRODUCTION
As reported in the literature, up to 12% of all COVID-19 patients may need intensive care unit admission for severe interstitial pneumonia, with possible long-term endotracheal intubation for mechanical ventilation and subsequent tracheostomy (Eur Arch Otorhinolaryngol. 2021;278:1–7). As is now known, prolonged endotracheal intubation can lead to mucosal injury and inflammation, granulation tissue formation, perichondritis, and subsequent stenotic scar tissue development. Moreover, tracheostomy may add trauma to the already damaged tracheal lumen, for example tracheal ring fracture, collapse, necrosis, malacia, and superinfection (Acta Otorhinolaryngol Ital. 2022;42:99–105).
Explore This Issue
August 2023In this setting, laryngotracheal stenosis represents one of the most common complications of invasive ventilation and tracheostomy. In addition, the absence of accurate monitoring of the cuff pressure or the need to maintain it above 50 mmHg for clinical reasons and prone position ventilation might contribute to the mechanism underlying the stenosis (Acta Otorhinolaryngol Ital. 2022;42:99–105; Respir Med. 2018;13:34).
As predicted by the European Laryngological Society, the incidence of laryngotracheal stenosis in post-COVID-19 patients may increase and should not be underestimated (Eur Arch Otorhinolaryngol. 2021;278:1–7; Acta Otorhinolaryngol Ital. 2022;42:99–105). After intensive care unit discharge, patients with breathing difficulties must receive a targeted evaluation aimed at ruling out the possibility of iatrogenic laryngotracheal stenosis, because a respiratory distress syndrome might be misdiagnosed in these cases (Acta Otorhinolaryngol Ital. 2022;42:99–105).
Regarding the treatment, Piazza et al state that tracheal resection and anastomosis represent an effective treatment in post-COVID-19 laryngotracheal stenosis patients (Acta Otorhinolaryngol Ital. 2022;42:99–105). Indeed, this strategy is common in the setting of previous prolonged intubation or tracheostomy, since external or internal trauma to the airway is associated with cartilage injury and the potential loss of structural support (Respir Med. 2018;13:34).
The purpose of the present paper is, therefore, to show step by step the tracheal resection anastomosis type A1, according to the University of Brescia classification (Acta Otorhinolaryngol Ital. 2022;42:99–105), in a post-COVID-19 patient. In addition, on the day of the surgery, the airway was managed with a new device, the Tritube with an outer diameter of only 4.4 mm. Here, we report the clinical case of a 62-year-old patient who presented to our attention for significant exertional dyspnea, cough, and sometimes dyspnea at rest.
Surgical Technique
The patient had been intubated for 21 days for severe COVID-19 interstitial pneumonia. Then, he had undergone a percutaneous tracheotomy for difficult weaning from ventilation in January 2021. The patient recovered in February 2021 with removal of the endotracheal cannula. The patient otherwise had no major comorbidities.
Three months after discharge and removal of the cannula, the patient began to complain of dyspnoea on exertion and occasionally at rest. He came to our attention about a year later. On fibroscopy, normal vocal cord motility was visualized, but a grade II tracheal subglottic stenosis (50%–71%), according to the Myer-Cotton airway grading system, at the site of a previous tracheotomy. The patient underwent a computed tomography (CT) neck scan, which showed a narrowing of the airway between the third and fourth tracheal rings.
Results from the literature state that, when feasible, tracheal resection and reconstruction is the treatment of choice in cases of benign tracheal strictures (Respir Med. 2018;13:34; Ann Thorac Surg. 2015;99:447–453). Therefore, considering the scarring and inveterate nature of the stenosis, our patient was a candidate for tracheal resection–anastomosis surgery. Airway management in such cases presents a particular challenge to anesthesiologists, so we elected to use the Tritube tracheal tube (Acta Anaesthesiol Scand. 2017;61:580–589).
Awake optical fiber nasotracheal intubation was conducted after local anesthesia of the nose, larynx, and trachea. First, a guide wire was positioned in the airways; then the Tritube was railroaded in the trachea (Figure 1). The patient was placed in a supine position and the neck was hyperextended to facilitate the exit of the trachea from the thoracic inlet.
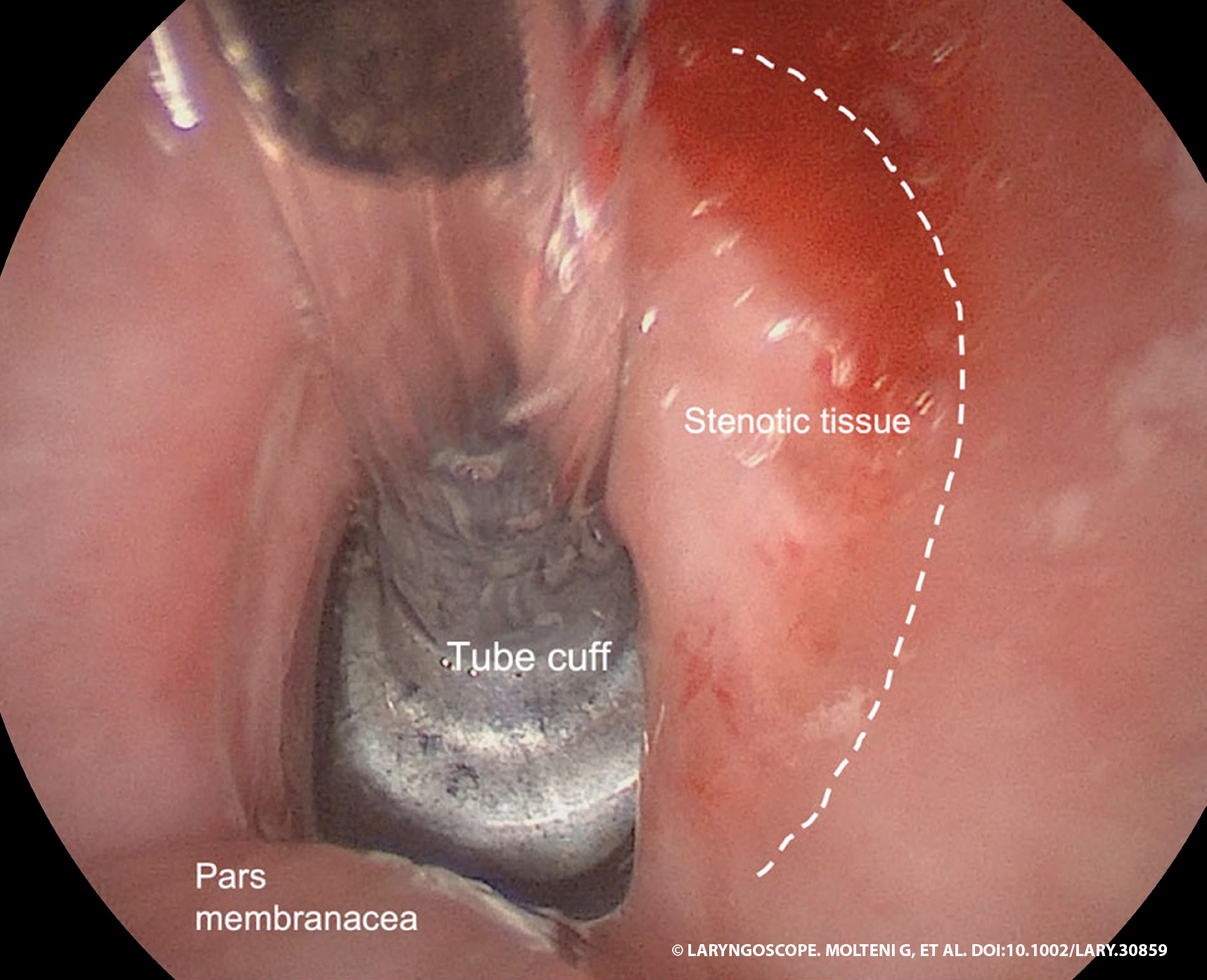
Figure 1. The Tritube is positioned, and the tube cuff is placed under the stenotic segment.
Step 1. A cervical collar incision was performed over the previous tracheostomy scar.
Step 2. Superior and inferior myocutaneous flaps were elevated, and the cervical fascia and prelaryngeal muscles were exposed.
Step 3. The prelaryngeal muscles and thyroid gland were dissected, with subsequent identification of pretracheal fascia and tracheal release for optimal mobilization.
Step 4. The length of the stenotic tract was measured; cranial and caudal incisions were made, obtaining a beveled shape of the two segments.
Step 5. End-to-end anastomosis with submucosal absorbable sutures 2–0 was performed. At the end of the surgery, the anastomosis was tested for air leaks.
Step 6. A collagen-coated sponge was placed on the suture. A layered closure of neck muscles and fascia was performed, with a drainage tube positioned before closure.
Before the suture, the head was mildly flexed to reduce anastomotic tension. It remained fixed with two strong chin–chest stitches in this position for five days postoperatively.
RESULTS
The patient was gradually woken up after the surgery in the intensive care unit, then transferred to the otolaryngology ward. Postop care involved bed rest with flexed head as abovementioned, and use of PPIs, laxatives, and cough sedatives. The patient was fed via nasogastric tube for the first three postoperative days and then gradually resumed oral feeding.
A CT scan was conducted at three and seven days postop to verify that there were no gas traces or blood collections in the peritracheal tissues. The patient was discharged after 10 days with no complications. The CT scan at 45 days after surgery showed an improvement in the narrowing of the airways.
In conclusion, using the procedure that is outlined here, we were able to obtain an improvement in the caliber of the patient’s airways and his symptoms with no complications.