Three months after discharge and removal of the cannula, the patient began to complain of dyspnoea on exertion and occasionally at rest. He came to our attention about a year later. On fibroscopy, normal vocal cord motility was visualized, but a grade II tracheal subglottic stenosis (50%–71%), according to the Myer-Cotton airway grading system, at the site of a previous tracheotomy. The patient underwent a computed tomography (CT) neck scan, which showed a narrowing of the airway between the third and fourth tracheal rings.
Explore This Issue
August 2023Results from the literature state that, when feasible, tracheal resection and reconstruction is the treatment of choice in cases of benign tracheal strictures (Respir Med. 2018;13:34; Ann Thorac Surg. 2015;99:447–453). Therefore, considering the scarring and inveterate nature of the stenosis, our patient was a candidate for tracheal resection–anastomosis surgery. Airway management in such cases presents a particular challenge to anesthesiologists, so we elected to use the Tritube tracheal tube (Acta Anaesthesiol Scand. 2017;61:580–589).
Awake optical fiber nasotracheal intubation was conducted after local anesthesia of the nose, larynx, and trachea. First, a guide wire was positioned in the airways; then the Tritube was railroaded in the trachea (Figure 1). The patient was placed in a supine position and the neck was hyperextended to facilitate the exit of the trachea from the thoracic inlet.
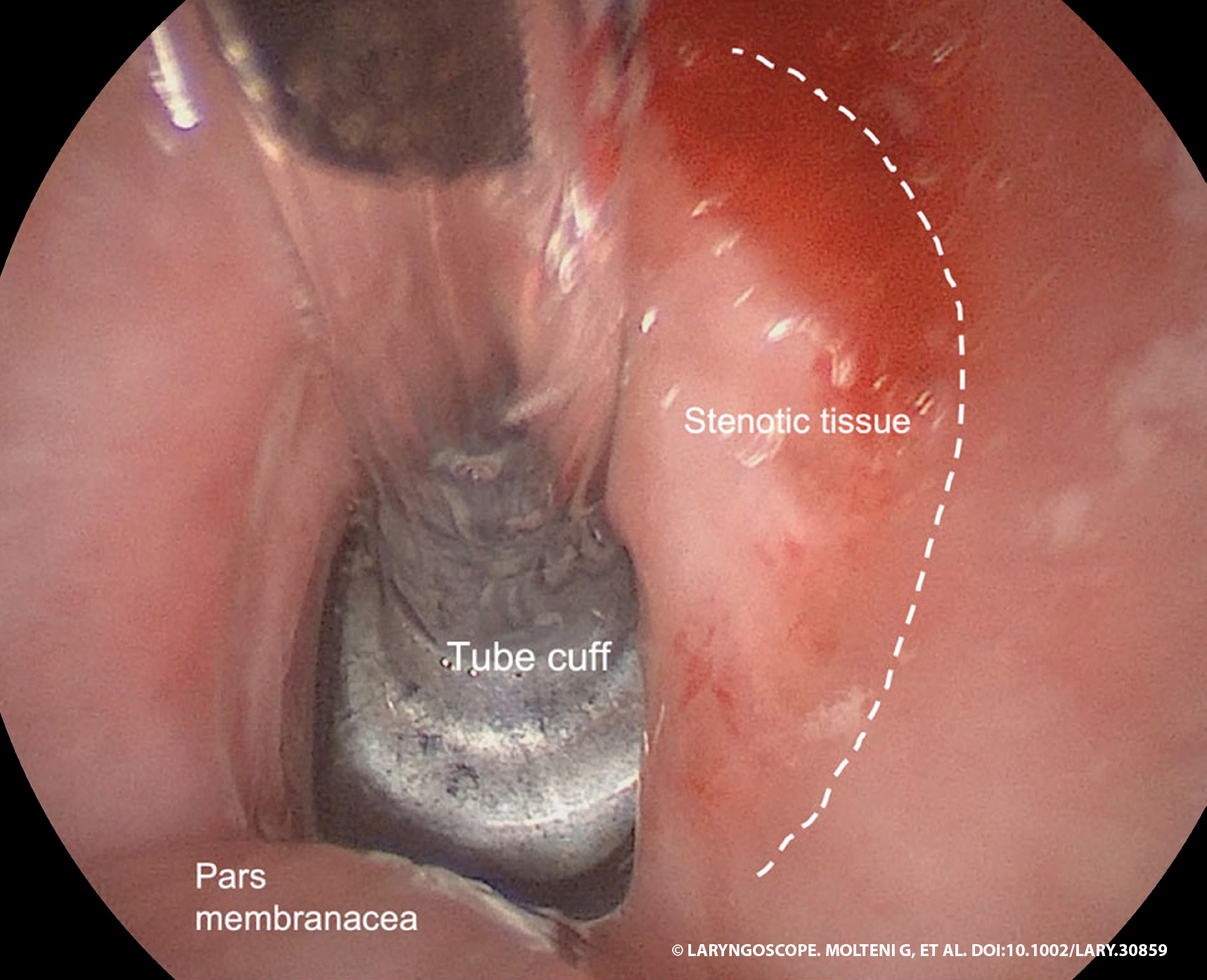
Figure 1. The Tritube is positioned, and the tube cuff is placed under the stenotic segment.
Step 1. A cervical collar incision was performed over the previous tracheostomy scar.
Step 2. Superior and inferior myocutaneous flaps were elevated, and the cervical fascia and prelaryngeal muscles were exposed.
Step 3. The prelaryngeal muscles and thyroid gland were dissected, with subsequent identification of pretracheal fascia and tracheal release for optimal mobilization.
Step 4. The length of the stenotic tract was measured; cranial and caudal incisions were made, obtaining a beveled shape of the two segments.
Step 5. End-to-end anastomosis with submucosal absorbable sutures 2–0 was performed. At the end of the surgery, the anastomosis was tested for air leaks.
Step 6. A collagen-coated sponge was placed on the suture. A layered closure of neck muscles and fascia was performed, with a drainage tube positioned before closure.
Before the suture, the head was mildly flexed to reduce anastomotic tension. It remained fixed with two strong chin–chest stitches in this position for five days postoperatively.