We chose a combined endoscopic and transoral approach for OAF closure consisting of a left classical maxillary antrostomy combined with minimally anterior medial maxillectomy using a double-layered flap based on a GPA flap and a BFP.
Explore This Issue
December 2022Nasal cavities were decongested with cotton pledgets soaked with adrenaline 1:10,000 and lidocaine 1%. The nasal septum, nasal floor, and head of left inferior turbinate were infiltrated with a solution of bupivacaine (0.25%) and epinephrine (1:100,000) following a subperichondrial and subperiosteal plane.
First, a left uncinectomy and middle meatal antrostomy were performed. Inflammatory mucosa and purulent discharge were removed using a curved aspirator and forceps. To ensure that no further disease was present, we inspected the maxillary sinus with a 30-degree scope.
A GPA flap was raised in the left nasal cavity. The distance from the anterior nasal spine to the incisive canal was 1.5 cm, measured previously on the patient’s CT, and it was pointed with a surgical marker on the nasal cavity. The posterior vertical incision was performed in the posterior limit of the septum descending across the junction of the soft and hard palate. The superior horizontal incision was performed parallel to the skull base, 1 cm below to preserve the olfactory epithelium.
The anterior vertical incision was performed along with the septal projection of the piriform aperture in an anterior oblique direction, and it was extended downward, 0.5 cm anterior to the GPA exit, to the floor and inferior meatus. Finally, an inferior horizontal incision was performed at the level of the inferior meatus joining both vertical incisions. The flap was elevated and preserved.
Afterward, a minimally left anterior medial maxillary approach was made to ensure an optimal handle of the maxillary sinus and GPA flap. A horizontal incision was made on the lateral nasal wall at the anteroinferior edge of the antrostomy, skirting the head of the inferior turbinate until reaching the piriform aperture. The resultant flap was elevated and displaced posteriorly. The exposed bone was drilled-out at 1–2 mm laterally of the piriform aperture, and then posteriorly in the inferior meatus preserving Hasner’s valve. Bone fragments were removed and a subtotal medial maxillectomy was performed with preservation of the inferior turbinate.
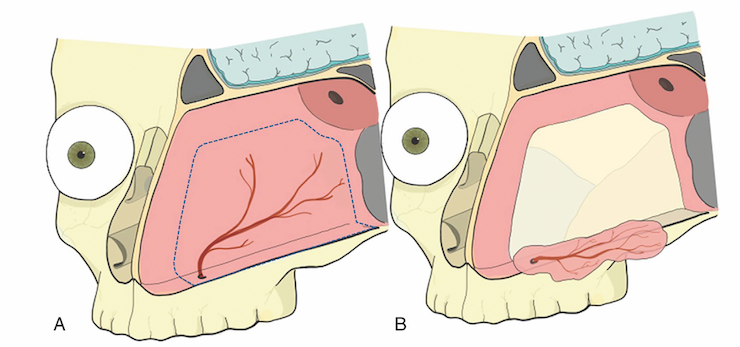
Figure 1. Schematic frontal view of oroantral fistula repair with a double-layered flap: greater palatine artery (GPA) pedicled flap and buccal fat pad flap (BFP). GPA pedicled flap covers left maxillary sinus’s floor and BFP is placed at 26 transorally.