INTRODUCTION
Pedicled endonasal flaps are currently the most widespread techniques with high success rate in the treatment of septal perforations (SPs) (Arch Facial Plast Surg. 2011;13:411-414). However, complete closure of large SPs (>2 cm) is technically more challenging, with a high risk of recurrence (Curr Opin Otolaryngol Head Neck Surg. 2012;20:58-65). Few endonasal flaps provide sufficient tissue for large SPs and usually are based on complex techniques or have a higher morbidity (Laryngoscope. 2018;128:1320-1327; Facial Plast Surg Aesthet Med. 2020;22:301-303). The anterior ethmoidal artery (AEA) flap is the most widely used endoscopic technique; however, it does not repair large SPs (Arch Facial Plast Surg. 2011;13:411-414).
The objective of this study is to describe step by step an innovative technique to repair large SPs with a pure endoscopic extended AEA flap, which includes the mucosa of sphenoid rostrum and the inferior meatus. In addition, we added a radiological study showing the additional area. This is the first report in the literature of an extended AEA flap.
METHOD
Surgical Technique. Six patients with symptomatic SP who underwent endoscopic repair with an extended AEA flap were included (see supporting video) (see Figure 1). The Ethics Committee of the Ramón y Cajal University Hospital in Madrid, Spain, approved the study, and all patients gave their signed informed consent.
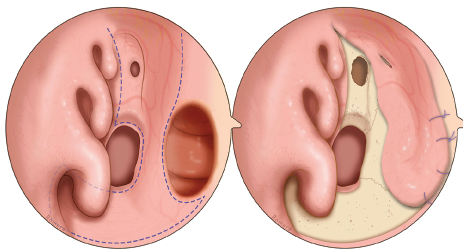
Figure 1. Schematic picture of the extended anterior ethmoidal artery (AEA) flap. (Left) Endoscopic view of the limits of the AEA flap, including the entire mucosa of the nasal floor and inferior meatus flap and the sphenoid rostrum. (Right) Endoscopic view of a large septal perforation completely repaired with the extended AEA flap suturing to the flap edges. The entire nasal floor, inferior meatus, and sphenoid rostrum are left denuded
The following technique was used:
- The nasal septum and nasal floor are subperiosteally or subperichondrially infiltrated with a solution of bupivacaine (0.25%) and epinephrine (1:100,000).
- Posterior incision: A vertical septal incision is made at the level of the junction of the perpendicular plate with the sphenoid rostrum. This incision descends involving all sphenoid rostrum mucosa. The incision continues through the choanal arch and the posterior septal border until it reaches the floor of the nostril. At that point, it runs through the junction of the hard and soft palate until it reaches the posterior limit of the inferior meatus.
- Anterior incision: The incision starts at the level of the middle turbinate and descends vertically through the nasal septum to the posterior edge of the SP. It continues anteroinferiorly to the anterior limit of the inferior meatus.
- Lateral incision: We join the anterior and posterior incision along the lateral limit of the inferior meatus without damaging the lacrimal duct valve.
- Once all incisions have been made, the entire mucosa of the inferior meatus, nasal floor, sphenoid rostrum, and remnant septal area are raised and rotated anteriorly until the SP is completely covered.
- The edges of the perforation are then refreshed and the flap is sutured to the remnant septal mucosa with absorbable stitches.
- Silicone nasal splints are fixed to the columella for three to four weeks.
Radiological Study. High-resolution craniofacial computed tomography (CT) scans (slices of 0.6 mm) of 150 nasal fossae were analyzed to measure the additional area provided by this extended AEA flap. These CT scans were obtained from 75 deidentified adults (all over 18 years of age) without any previous sinus or skull base pathology. The sphenoid rostrum and nasal floor and inferior meatus areas were measured using the open-source DICOM file viewer Horos.
RESULTS
Six patients with symptomatic SP who underwent endoscopic repair with an extended AEA flap were included (mean age 46.5 (36-66) years old, 50% female). The first patient, a 41-year-old woman, presented with a 3.5-cm SP due to orthognathic surgery 10 years ago. The second patient, a 66-year-old woman, suffered a 4-cm SP because of prior rhinoplasty and past history of cocaine abuse. Two other patients, a 45-year-old man and a 36-year-old woman, had an SP of between 3 and 3.5 cm due to a previous septoplasty. Two other patients, two men aged 45 and 46 years, suffered from bothersome symptoms due to a 3.5 cm SP secondary to past history of cocaine abuse without previous surgeries. Complete closure of the SP in all cases was achieved. Silicone splints were placed in all cases for four weeks. Follow-ups of 11.3 (16-8) months showed no evidence of recurrence.
In the radiological analysis, an average sphenoid rostrum area of 3.0 ± 0.5 cm2 and an average area of the floor and inferior meatus of 13.4 ± 1.9 cm2 were obtained. This technique provides an additional tissue of 16 cm2.