Surgical Technique
Explore This Issue
January 2023A combined transcervical and endoscopic endonasal approach to access the infratemporal fossa and parapharyngeal space was performed in all patients. A modified preauricular/transcervical incision was designed. The facial nerve was kept within the parotid parenchyma and elevated along with the parotid tail, rather than identifying the nerve and potentially creating a stretch injury from retraction on an unprotected nerve. The stylomandibular ligament was transected and the styloid process removed to the skull base, taking care to gently elevate the parotid in this area to protect the facial nerve within the parenchyma. Anterior retraction or ligation of the external carotid artery was performed to open the post-styloid parapharyngeal space. The ICA was identified, along with the glossopharyngeal, vagus, accessory, and hypoglossal nerves.
Next, the nasopharynx musculature, including the superior constrictor and Eustachian tube complex, were identified anteromedial to the great vessels. We dissected the previously identified ICA and nerves to the level of the skull base, while identifying signs of tumor involvement. At the level of the carotid canal, a 3-in. Cottonoid was placed medial to the carotid artery to provide a visual cue and protection during subsequent endonasal tumor dissection (Figure 1). With the ICA identified, protected, and lateralized relative to the tumor, endonasal endoscopic tumor dissection was conducted via a transpterygoid approach to access the pterygomaxillary and infratemporal fossae. We accomplished this by performing a medial maxillectomy followed by identification and ligation of the sphenopalatine artery.
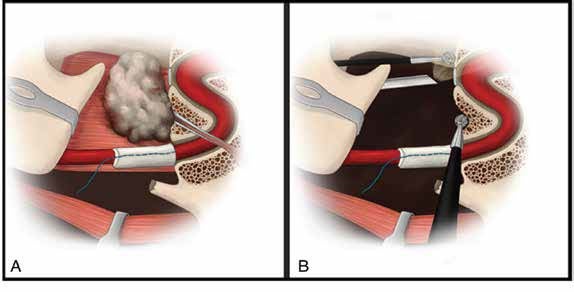
Figure 1. (A) Styloid ligament has been transected and a Cottonoid pledget placed on the internal carotid artery for protection during tumor resection. The tumor lies in the nasopharynx, obstructing the Eustachian tube. (B) Endoscope and instrument accessing nasopharynx via the nares with additional instruments entering nasopharynx via the lateral, transcervical access.
Then, the pterygoid plates were identified and resected for access to the anteromedial boundaries of the tumor. The pterygomaxillary fissure was then resected. The posterior extent of dissection was dictated by tumor involvement. After endonasal mucosal cuts were completed, the superior constrictor attachments to the skull base were released from both the endonasal and lateral approach, revealing the foramen lacerum and foramen ovale. The endonasal tumor dissection ultimately communicated with the cervical incision around the specimen, and either the endonasal or the cervical access could be used to complete tumor extirpation. With the carotid canal and foramen lacerum in full view, we were able to transect the Eustachian tube using the lateral approach as it entered its bony canal. In all cases, either reconstruction with regional pedicled flap or free tissue transfer was used to close the nasopharyngeal defect (see the supporting video).