INTRODUCTION
Advances in endoscopic techniques have spurred the growth of awake in-office outpatient laryngeal procedures. Targeted applications of local anesthesia need to be effective because the common limiting factor for performing these procedures is patient tolerance (J Voice. 2019;33:732-746). For many patients who require multiple interventional treatments of the larynx and especially those at risk of being put under general anesthesia, awake in-office procedures may be the preferred treatment method.
The posterior larynx, characterized by a rich network of sensory endings, is a problematic area to anesthetize and treat. Sensory reactions of the laryngeal adductor reflex result in laryngospasm, which decreases precision and increases complications or failure of the awake operation. One reason may be related to dual innervation by sensory fibers from the recurrent laryngeal nerve and the superior laryngeal nerve forming the interneural communications of the arytenoid plexus and Galen’s anastomosis (Laryngoscope. 2012;122:865-867). Also, the range of motion and velocity of the posterior larynx in the region of the arytenoid and interarytenoid is significantly greater than the anterior commissure. Treatment of the posterior glottis, such as laser ablation and therapeutic injection, is challenged by patient tolerance and limits the application of in-office awake procedures. In addition to standard patient preparation and anesthetization, we describe direct injection of local anesthetic into the posterior glottis to induce a temporary selective unilateral adductor vocal cord paresis allowing for increased patient tolerance of awake in-office treatment.
There are several methods of achieving local or regional anesthesia for awake laryngeal procedures. Topical anesthesia methods include a nebulized anesthetic, gargles, dripping of anesthetic superior to the larynx through the working nasolaryngoscope channel, and transtracheal lidocaine injection. Unilateral and bilateral superior laryngeal nerve blocks are also common local and regional anesthesia methods for laryngeal procedures.
METHOD
We describe an anesthetic technique using direct intramuscular lidocaine injection to induce temporary adductor paresis and sensory loss. We most commonly use this method for patients with recurrent disease near the interarytenoid and arytenoid regions.
Operative Technique
The patient is seated in the upright position, and lidocaine hydrochloride (HCl) 2% and oxymetazoline HCl 0.025% spray are administered to the nasal cavity for topical anesthesia and vasoconstriction. The oropharynx and larynx are further anesthetized with a laryngeal gargle of lidocaine HCl 4% 40 mg/mL (4% lidocaine) and/or butamben-tetracaine-benzocaine 2%–2%–14% 200 mg/sec (cetacaine). A supplemental 2 cc of 4% lidocaine is often delivered via transtracheal approach using a 23-gauge needle.
Under direct visualization via a nasopharyngoscope held by an assistant, the 2.0-inch 25-gauge needle, prepared with the double- bend technique, is passed through the thyrohyoid membrane just superior to the thyroid notch to enter the endolarynx (Laryngoscope. 2021;131:E1580-E1588). The two intramuscular targets most frequently injected are the thyroarytenoid/lateral cricoarytenoid (TA/LCA) muscles and the interarytenoid (IA) muscle (also referred to as the transverse arytenoid). The TA/LCA injection is placed lateral and deep to the vocal process of the arytenoid (Figure 1). The interarytenoid muscle injection is placed at the junction of the interarytenoid region and arytenoid, inferior to the vocal process. A volume of 1 ml 1% lidocaine with epinephrine is injected into one or both areas. After several minutes, reduced mobility of the true vocal fold is confirmed with a nasopharyngoscope.

Figure 1. An alternative approach targeting the thyroarytenoid muscle is placed deep and lateral to the vocal process of the arytenoid. This injection is most frequently used for vocal process lesions such as granulomas.
After completion of the therapeutic treatment, the patient is observed for 30 minutes in the clinic and instructed to follow nothing-by-mouth instructions for 90 minutes. Modifications for this procedure include using a longer 2.5-inch 25-gauge needle to reach the IA region for tall patients, patients with an increased neck circumference, adipose tissue, or altered anatomy due to previous surgical treatment or radiation. The transcricothyroid approach can also be used for IA muscle injection. Observation has shown that sometimes sufficient anesthesia is obtained through a single injection around the arytenoid, usually in the vicinity of the area of treatment (Figure 2).
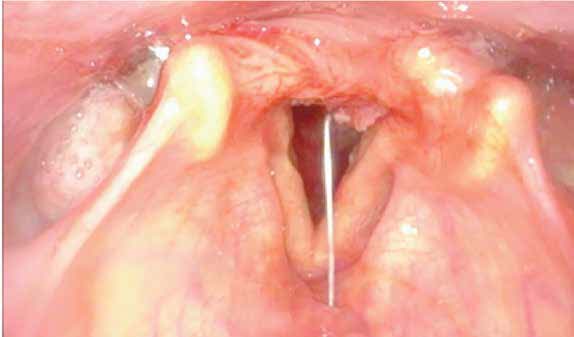
Figure 2. Injection into the interarytenoid muscle to limit adduction. The needle tip is rotated so that the injection is concentrated on the left side.
RESULTS
This technique has been utilized for patients with lesions of the posterior larynx, including recurrent respiratory papillomatosis, leukoplakia, posterior glottic stenosis, and granulomas. Office-based procedures are the preferred method for administering serial treatments for highly recurrent or rapidly progressive diseases within our practice (see supplemental video).