INTRODUCTION
Different endoscopic techniques to repair septal perforations (SP) using pedicle endonasal flaps (PEF) have been developed in recent years. Anterior ethmoidal artery flaps, including the simple and the extended (eAEA), and greater palatine artery (GPA) flaps are widely used procedures with a success rate exceeding 90% (Laryngoscope. 2022;132:298–300; Eur Arch Oto-Rhino-Laryngol. 2021;278:2115–2121). The inverted edges (EE) flap is a mucosal flap rotation technique, in which the edges of the SP are raised and rotated to the contralateral side of the nasal cavity (Int J Pediatr Otorhinolaryngol. 2020;130:109817).
Anterior SPs are technically challenging, with a higher risk of recurrence, especially those that have their upper edge in a high position (Curr Opin Otolaryngol Head Neck Surg. 2012;20:58–65). The objective of this study is to describe the combination of a partial EE with a PEF (eAEA or GPA), in which the anterior incision includes the contralateral mucosa. We believe that the combination of both techniques can be useful for the anterior closure of SP, especially in those in which the anterior edge of the perforation reaches the skin of the columella.
METHOD
Surgical Technique
The zigzag flap incision: The nasal septum and nasal floor are infiltrated with a solution of bupivacaine (0.25%) and epinephrine (1:1,000,000). For an eAEA, a posterior vertical septal incision is made at the level of the junction of the perpendicular plate with the sphenoid rostrum. The incision descends, involving all the sphenoid rostrum mucosa, and continues through the choanal arch and the posterior septal border until it reaches the floor of the nostril, then runs through the junction of the hard and soft palate until it reaches the posterior and lateral limit of the inferior meatus (Figure 1A). If a GPA is performed, the posterior vertical septal incision is performed 1 cm inferior to the olfactory sulcus, then is prolonged from the septum across the junction of the soft and hard palate to the inferior meatus.
The anterior incision starts at the level of the middle turbinate and descends vertically through the nasal septum, until it reaches the postero-superior edge of the SP. At this point, it continues toward the contralateral nostril with a posterior direction, and then descends toward the inferior–posterior border of the SP, obtaining mucosa posteriorly to the posterior edge of the SP in the contralateral nostril. Subsequently, it runs toward the inferior–anterior border, gaining mucosa inferiorly to the inferior edge of the SP (Figures 1A, 1B). At that point, the incision goes back to the initial nostril, going toward the floor and later reaching the anterior limit of the inferior meatus. A lateral incision joins the anterior and posterior incisions along the lateral limit of the inferior meatus.
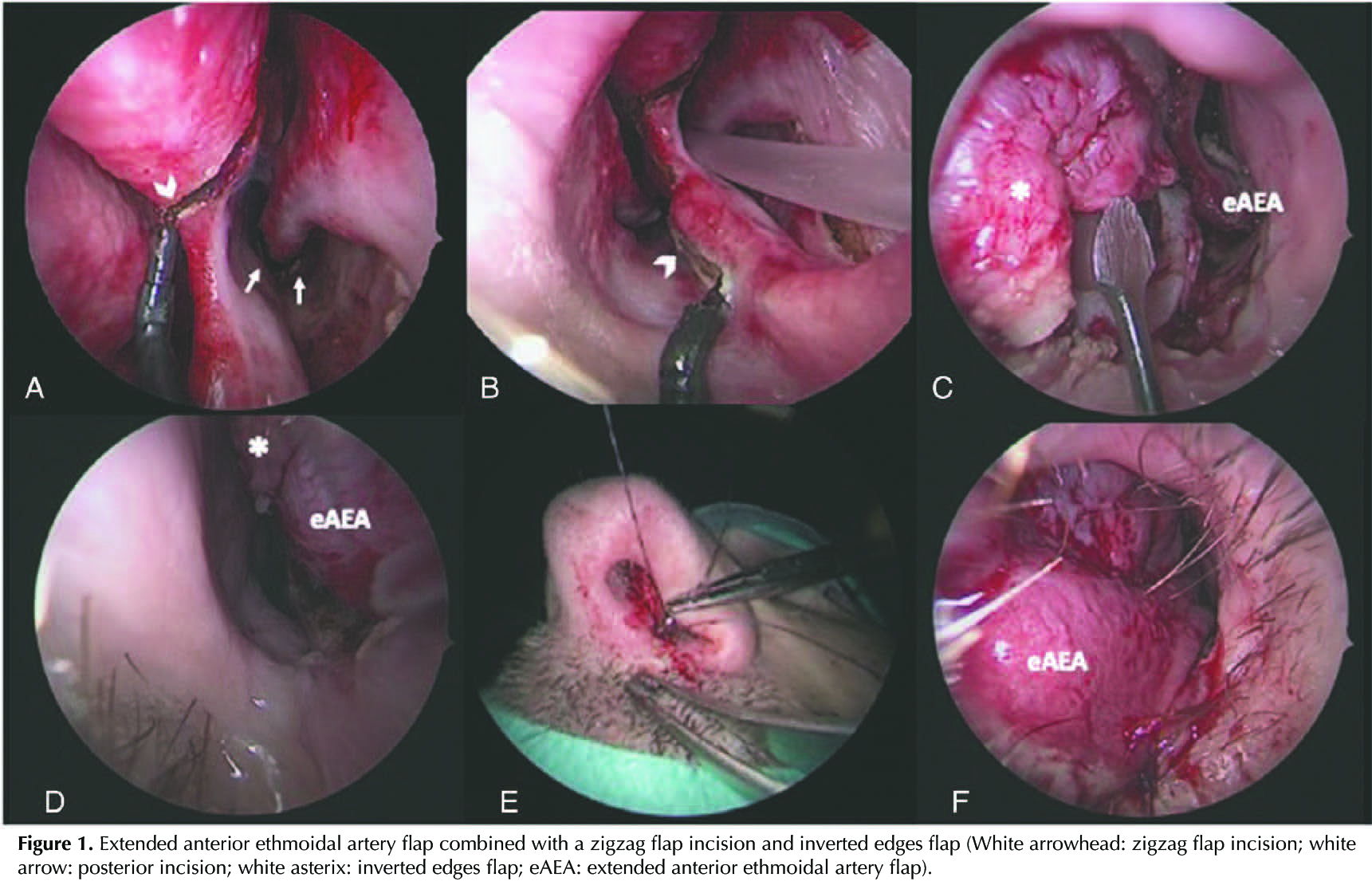
Once the SP edges are turned, and the size of the perforation has decreased at the expense of its most superior and anterior edge (Figures 1D, 1C), the PEF is rotated and placed until the perforation and the inverted edges are completely covered (Figures 1F, 1D). Two stitches are placed in the most anterior and superior part of the flap (Figure 1E). Silicone nasal splints are fixed to the columella for three to four weeks.
RESULTS
Four patients from Centro Médico Teknon and Hospital Clinic of Barcelona were included in this study. The mean age was 43 years. The cause of the SP was secondary to drug abuse (cocaine) in three cases and nose picking in one patient. An eAEA was used in three cases and GPA was performed in one patient due to the posterior edge of the SP being anterior to the incisive channel. All the patients had a complete closure of the perforation six months after surgery.
Although this is a small case series and the follow-up time was only up to 13 months, our results show that the use of EE in combination with the anterior zigzag incision for PEF can be useful tools that could be considered when performing a surgical closure of anterior SP. This technique is limited to SP with osseocartilaginous support and a complete epithelialization of the perforation margins.