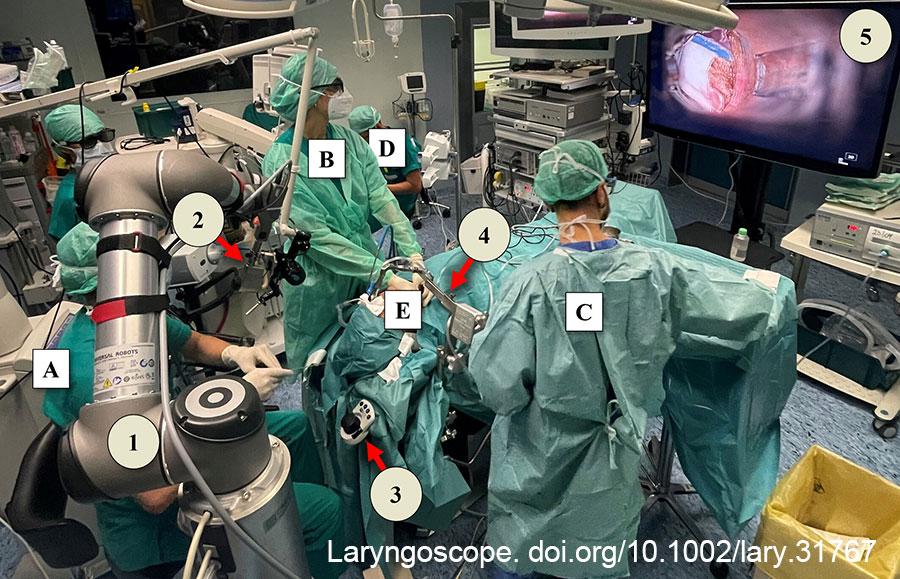
Figure 1. Operative theatre setup during TOLES, with the position of the surgeon and his team (letters) and the TOLES tools (numbers). (A) surgeon; (B) assistant surgeon; (C) scrub nurse; (D) anesthesiologist; (E) patient; 1, ARTip Cruise robotic arm; 2, VITOM 3D-HD Exoscope coupled to the laser micromanipulator; 3, VITOM IMAGINE1 PILOT; 4, suspension system with Zeitels Suspension Gallows (Endocraft LLC, Boston, Mass.) and DEDO laryngoscope (Karl Storz, Tuttlingen, Germany); 5, 3D monitor. TOLES = transoral laser exoscopic surgery.
We proposed the employment of CO2 TOLES as an alternative to CO2 TOLMS in the treatment of supraglottic cancer located in the supra-hyoid portion of the epiglottis and extended to the infra-hyoid epiglottis and to the left aryepiglottic fold (cT2N0). Endoscopic results, evaluated during follow-up (the latest control has been performed two years after surgery), showed excellent healing of the surgical field without any macroscopic evidence of residual disease. Laryngeal phonatory and swallowing functions were completely preserved.
Explore This Issue
January 2025In our experience, CO2 TOLES proved feasible for early intermediate laryngeal SCC and represents a valuable alternative to TOLMS. The 3D visualization helped the surgeon and assistant to dominate the tumor at 360° and achieve en bloc removal within free resection margins and with optimal post-operative results. Moreover, CO2 TOLES provides a didactic gain, with the subjective benefits of ergonomics and optimal intra-operative visualization being well perceived throughout the entire surgical procedure (Fig 1).