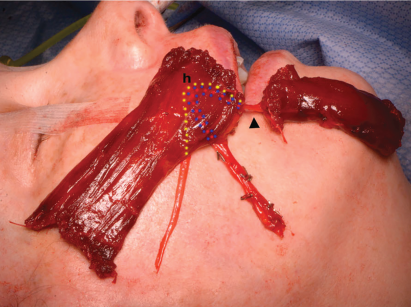
Fig. 1. Intraoperative photograph of harvested ipsilateral flap demonstrating orientation of upper and lower lip paddles following 180° in-plane rotation. In this iteration, the nerve and vascular pedicle are reflected deep to the flap for coaptation with the ipsilateral nerve-to-masseter muscle and anastomosis with the facial vessels. The approximate location of the hilum (h) and course of the neurovascular pedicle (dotted lines: yellow—nerve-to-gracilis muscle, blue—venae comitans, red—artery) on the deep aspect of the flap is demonstrated, together with the continuation of the neurovascular pedicle (arrowhead) to the lower lip paddle.
© Ein, et al. Laryngoscope.
Introduction
Smile reanimation techniques pioneered by Gillies (Proc R Soc Med. 1934;27:1372-1382) and Harii (Plast Reconstr Surg. 1976;57:133-143) reliably restore oral commissure excursion, though ideal results are uncommonly achieved without intact lower lip depressor function. In 1995, Ueda described concurrent segmental transfer of latissimus dorsi and serratus anterior muscles for restoration of lower lip depressor function with smile reanimation (Plast Reconstr Surg. 1995;95:1288-1296). In 2015, Biglioi characterized a similar approach using a dual-paddle latissimus dorsi muscle flap (BMJ Case Rep. 2015:bcr2015210436). Herein, we characterize a dual-paddle gracilis muscle flap based on a single neurovascular pedicle for rehabilitation of dental display smile. One paddle elevates and lateralizes the upper lip and commissure, while the second paddle depresses the lower lip.
Method
Two adult females (ages 50 and 65) with long-standing unilateral postparalytic facial palsy underwent uncomplicated dual-vector gracilis muscle transfer in accordance with institutional review board protocols. Preoperative examinations demonstrated midfacial hypertonicity with upper lip ptosis, restricted oral commissure excursion, and superiorly-malpositioned lower lip with smile. A facial flap is elevated atop the temporoparietal fascia superiorly, and below the superficial musculo-aponeurotic system (SMAS) inferiorly via a preauricular incision with temporal and cervical extension. The donor neurotization source is isolated. Absorbable sutures are parachuted along ipsilateral orbicularis oris muscle fibers between the modiolus and philtral column. A mucosal incision is made oral to the wet-dry junction of the ipsilateral lower lip and joined to a cutaneous submental crease incision by tunneling in the sub-SMAS plane medial to the mental foramen. The sub-SMAS lower lip and cheek spaces are joined superior to the mental foramen, and the ipsilateral facial vessels prepared for microvascular transfer.
An ipsilateral dual-paddle gracilis muscle flap is harvested via a 6-cm thigh incision. Dissection is carried through subcutaneous fat and fascia overlying the adductor longus muscle. The neurovascular pedicle is visualized and released from fascia overlying the adductor magnus muscle. The anterior two thirds of the muscle is freed along a 12-cm length whose superior extent is 2 cm above the neurovascular pedicle hilum. The muscle segment is released inferiorly using bipolar scissors, and laterally by sharp dissection from the adductor magnus muscle. The superficial surface is debulked, and the flap divided longitudinally via meticulous skeletonization of the neurovascular pedicle connecting the two segments to enable their 135° separation. Running locking absorbable suture is placed along superior and inferior edges of the anterior segment to serve as pseudotendons. The nerve-to-gracilis muscle (NTG) is transected at its branch point from the anterior division of the obturator nerve. Flap vessels are dissected and ligated at their profunda femoris vessel origin. The leg incision is closed in multiple layers over a suction drain, and compression wrap placed.
One paddle elevates and lateralizes the upper lip and commissure, while the second paddle depresses the lower lip.
The flap is transferred with 180° in-plane rotation, placing the hilum of the neurovascular pedicle at the philtrum (Fig. 1). The upper lip paddle is inset medially. The vascular pedicle is reflected under the flap and anastomosed to the facial vessels. The second paddle is delivered into the lower lip pocket, trimmed to length, and inset at neutral tension using absorbable sutures to orbicularis oris fibers and periosteum of the lower mandibular border. The temporoparietal fascia is incised lateral to Pitanguy’s line, and the upper lip paddle secured to the true temporalis fascia at neutral tension using absorbable sutures. The NTG is reflected under the flap for coaptation with the ipsilateral nerve-to-masseter muscle, or alternatively tunneled across the upper lip for cross-facial neurotization. The facial flap is redraped, and incisions closed using absorbable sutures over a suction drain.
Results
Patients were admitted two nights for monitoring; no complications arose. At the six-month follow-up, bite-driven smile demonstrated improvement in oral commissure excursion and active lower lip depression, with favorable upper dental display. Open-source facial analysis software was employed for quantification of surgical outcomes. In the first patient, oral commissure excursion with full-effort smile with teeth in occlusion improved from 30.34 mm on the affected side to 36.9 mm (vs. 35.6 mm on the unaffected side), and average lip opening (dental show) on the affected side improved from 0.8 mm to 6.7 mm. In the second patient, oral commissure excursion with full effort smile and teeth occlusion improved from 28.0 mm on the affected side to 37.2 mm (vs. 35.3 mm on the unaffected side), whereas average lip opening on the affected side improved from 1.3 mm to 5.3 mm.