Introduction
Microtia, the absence or underdevelopment of the auricle, is thought to affect 1 in 5 to 10,000 live births worldwide and has been associated with significant psychosocial morbidity that may dramatically improve following surgical repair (Facial Plast Surg Clin N Am. 2016;24:577-591). Currently, these techniques largely fall into two major categories: autologous reconstruction using costal cartilage, and synthetic reconstruction using a porous polyethylene (PPE) construct. There is considerable debate regarding the superior technique for various clinical settings in which to apply these differing methods. Nonetheless, both techniques aim to create a reliable construct for the novel auricular framework, which is then covered with native tissue (skin, fascia, or both). For the purpose of discussion in this paper, the senior author primarily performs the porous polyethylene-based reconstruction.
Microtia can present in isolation or as part of a syndrome such as oculo-auriculo-vertebral syndrome (OAVS), which encompasses Treacher Collins and Goldenhar syndromes. Patients with OAVS may be distinguished by the presence of hemifacial microsomia, the underdevelopment of the bony and soft tissue structures of one or both sides of the face with resulting facial asymmetry. These patients have a host of unique anatomical abnormalities that present surgical challenges and often preclude favorable aesthetic outcomes following reconstructive surgery (Plast Reconstr Surg. 2018;142:1558-1570). Associated abnormalities can include asymmetric malar height and projection, mandibular hypoplasia, and a deficient mastoid, among others. Failure to recognize and address these deficiencies can lead to obvious asymmetries and poor aesthetic outcomes.
A common problem seen postoperatively in this subset of patients includes underprojection of the lower third of the ear, most notable when seen in frontal view. This asymmetry likely results from undercorrection of mastoid hypoplasia, resulting in decreased projection of the lower third of the ear. Despite multiple studies intending to determine ideal angles and size of the reconstructed ear, this particular measure has not been described in the literature to our knowledge. Referred to as the axis of projection (AOP), this measurement represents an angle seen on frontal view formed from the superior helix of the ear (vertex) bisecting the lobule in a vertical axis. Given the importance of this angle in relation to the aesthetic outcome of surgery, different methods to achieve symmetry were explored and described herein.
An increasingly popular tool used across multiple surgical specialties is three-dimensional (3D) printing, which offers the opportunity for case-by-case customization. This is particularly useful during surgical planning and can help the surgeon better understand each patient’s unique anatomy. Within the field of microtia reconstruction, these types of 3D models have been utilized to help train future microtia surgeons, while other groups have attempted to integrate 3D printing into the creation of a modifiable implant for the day of surgery (Otolaryngol Head Neck Surg. 2017;156:999-1010).
Matching the axis of projection when reconstructing the microtic ear allows for the optimization of aesthetic outcomes, in particular along the frontal view.
This manuscript aims to address the difficulties presented with microtia repair in patients with hemifacial microsomia. We discuss our approach to preoperative planning as well as our intraoperative technique, focusing on descriptive measures that are important to identify at the time of surgery to maximize cosmetic outcomes.
Method
The following method was applied to six consecutive cases for:
Preoperative Planning: Patients scheduled for microtia repair underwent thincut computed tomography scans that specifically included the entirety of both ears and surrounding soft tissue. These scans were uploaded into Mimics and Autodesk Meshmixer to create digitally manipulatable models, allowing for measurements of mastoid and midface deficiency. Virtual images were used to create 3D-printed models for physical manipulation (Figure 1).
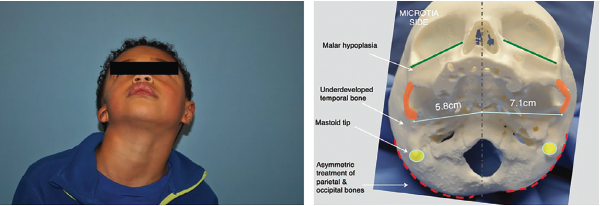
Figure 1. Left: preoperative image demonstrating degree of hemifacial microsomia highlighted by deficient mastoid and asymmetric midface and mandible. Right: 3D-printed skull highlighting these changes at the bony level.
© Laryngoscope. Kimura, et al.doi:10.1002/lary.29823
Using the 3D-printed model, a standard PPE implant was placed while visualizing the contralateral ear at different angles. Ideal positioning was based on a location that achieved the greatest amount of symmetry to the contralateral ear in three dimensions, including both the height of the upper third of the ear (on profile and frontal views), anterior/posterior positioning (profile), and projection of the lower third of the ear (frontal).
Once ideal positioning was determined, a silicone putty mixture was placed onto the model and manipulated by adding or removing material to support the position of the PPE implant at the ideal AOP. At that point, the silicone was allowed to harden. Next a 3-mm punch biopsy tool was used to take measurements at three separate places on the mold (helical root, common crus, and the base of the conchal bowl). This process was repeated an additional two times to ensure consistent measurements.
Once ideal position and augmentation of the ear were determined, facial landmarks were sketched onto clear plastic as a template for intraoperative positioning. Landmarks included the microtic ear, lateral canthus, lateral nasal sidewall, alar crease, and oral commissure. This process effectively created a template mask to help replicate placement (in two dimensions) on the day of surgery, while the depth of the silicone putty mold measurements determined projection in 3D of the lower third of the ear.
Intraoperative Application: On the day of surgery, the template mask previously created during preoperative planning was used to mark the ideal placement of the ear. This was performed prior to sterilization and draping of the patient. Next, the template was placed between two sterile transparent dressings, which allowed for frequent verification of positioning once a sterile field was created. The measurements taken from the silicone wedge during the preoperative planning session were used to augment the PPE auricular framework (by adding from a separate PPE block) and appropriately project the lower third of the ear.
Patients were routinely seen in follow-up three to five days postoperatively for removal of a protective head dressing, and again one week later for removal of silicone casting material secured over the neo-auricle. Intralesional corticosteroid was injected as needed at the surgeon’s discretion around three to four weeks later to areas that appeared to demonstrate excessive edema. Patients were instructed to protect the ear at night with the use of a removable silicone cast for several weeks.
Results
Hemifacial microsomia presents a unique challenge in microtia repair due to the particular anatomic abnormalities that result from a deficient mastoid and asymmetric midface. This study aims to introduce a new concept, the AOP, which should be identified in all patients with hemifacial microsomia undergoing microtia repair. Matching the AOP when reconstructing the microtic ear allows for the optimization of aesthetic outcomes, in particular along the frontal view. We describe a 3D imaging protocol that can be useful in predicting the degree of mastoid deficiency present, and can help augment the lower third of the neo-auricle to accommodate this deficiency. As technology continues to improve, it is important for the field of facial plastics and reconstructive surgery to rely more on quantitative data and calculable measurements in order to achieve optimal outcomes more consistently.