The process of obtaining informed consent from a patient is among the thorniest legal issues an otolaryngologist faces when managing surgical procedures. However, Jeffrey Wolf, MD, believes the process can be easy to start; specifically, he recommends that physicians begin by looking a patient in the eye, at his or her level.
Explore This Issue
January 2017“Something I always do when I’m talking to a patient about surgery … I always sit down,” said Dr. Wolf, associate professor and associate chair of clinical practice of otorhinolaryngology-head and neck surgery at the University of Maryland School of Medicine in Baltimore. “I’m never standing; I never want them to feel like I’m rushed. I always sit down, because if you sit down for two minutes, they feel like you spent a lot more time with them than if you stood up.”
Time and effort might be the two most important factors in establishing a rapport with a patient that helps ensure that the informed consent process works as intended, Dr. Wolf said. And informed consent is just that—a process that needs to be honed to make sure patients are truly informed.

© Bacho / shutterstock.com
Why is informed consent so important? Research presented in 2007 found that between 1985 and 2005, 37% of all malpractice claims involving endoscopic sinus surgery (ESS) also involved informed consent (Am J Rhinol. 2007;21:584-590). Furthermore, the researchers found that 16% of all otolaryngology malpractice claims centered on informed consent. More recently, of the 48,589 malpractice claims reported to the PIAA (formerly known as the Physician Insurers Association of America) Data Sharing Project between 2010 and 2014, 12,865 (28%) resulted in payment to the plaintiff. Additionally, 740 named an otolaryngologist in the claim, with 298 (40%) of those resulting in payment to the plaintiff.
“It is higher than what the broader community is, which prompts us to ask what variables contribute to these cases resulting in higher payment,” said Divya Parikh, MPH, PIAA’s vice president of research and risk management.
The numbers only get worse for surgical procedures that involve the nasal region. Malpractice claims reported to the PIAA for these procedures over the five-year period from 2010 through 2014 totaled 311, and approximately half of those resulted in payment.
Traditionally, in medicine, we think of informed consent as a piece of paper that the patient signs, but that’s not what informed consent is. Informed consent is actually the discussion around surgery and the process by which that piece of paper is signed. —Leigh Sowerby, MD
What Is Informed Consent?
The medical–legal implications of informed consent are often misunderstood, according to Leigh Sowerby, MD, assistant professor in otolaryngology-head and neck surgery at Western University in London, Ontario, in Canada. “Traditionally, in medicine, we think of informed consent as a piece of paper that the patient signs, but that’s not what informed consent is,” he said. “Informed consent is actually the discussion around surgery and the process by which that piece of paper is signed.”
Dr. Sowerby said the process of obtaining informed consent has four main components, as established in the landmark legal decision Schloendorff v. Society of New York Hospital (1914). According to this decision, to give consent, a patient must understand the following:
- The nature of the disease or condition;
- The benefits and the risks of the procedure;
- The alternatives to the procedure; and
- The consequences of no action.
Dr. Sowerby acknowledged that it can be tough in a busy practice to have a thorough discussion of all of those components with a patient, to the point where you’ve answered his or her concerns. “As an example, we all have our little spiel that we give when we take consent for a specific procedure. … If you’re a patient and you’re hearing that and you hear “heart attack,” and you get stuck on heart attack, you miss all of the other stuff that’s discussed during that consent. And you end up signing the piece of paper because you know you have five or 10 minutes with the physician. But you may not have had all of your concerns addressed, and you definitely don’t remember everything that was discussed.”
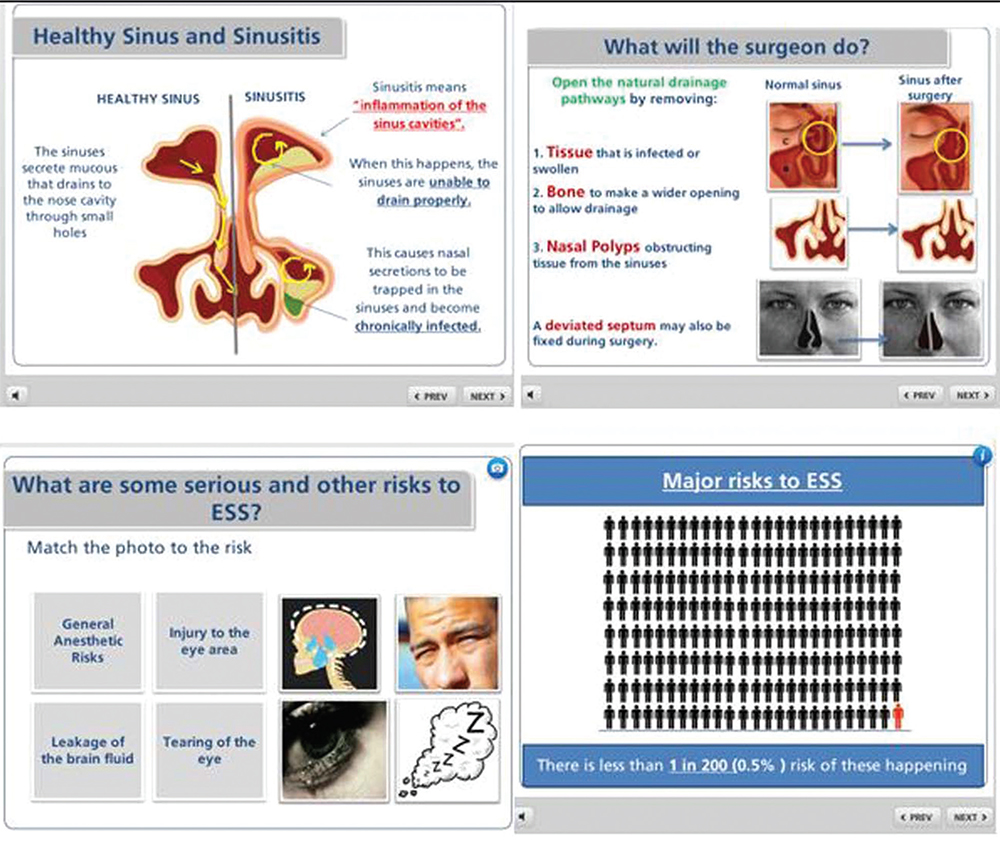
In June 2016, Dr. Sowerby and his colleagues published a paper in The Laryngoscope on the process of informed consent for ESS (Laryngoscope. 2016;126:1273–1278). The researchers found an early improvement in overall risk recall in patients who finished an interactive multimedia module (see Figure 1). The report concluded that it is important to integrate multimedia tools into the otolaryngologist’s armamentarium for clinical practice. “Simple, interactive multimedia education modules offer a cost-effective, efficient, and effective platform to supplement the traditional informed consent process,” they concluded.
(click for larger image)
Figure 1. Screenshots of Dr. Sowerby’s multimedia module for patient consent. Audio voice-over, images, and relevant figures were synchronized to convey clinical information. Animations were used to describe visual phenomena. To optimize patient comprehension, the module contained information at the eighth grade level and incorporated large fonts, bulleting, bolding, and underlining, as well as graphic displays using pictographs of risks and benefits. The module was designed to be interactive to let the patient control the information flow rate.
Credit: The Laryngoscope. ©The American Laryngological, Rhinological and Otological Society, Inc.
“The thing I like about the multimedia slideshow we have created is that it gives us control of what patients are seeing,” Dr. Sowerby added. “Sometimes patients don’t feel duly informed, and if they don’t, they’re going to do a Google search, and they’re going to see what shows up there, and they may or may not be reading things that are A) factual or B) realistic to their specific case. So, having some control over that, I think, is beneficial. It lets us ensure that the discussion is [going] in the direction it needs to be for that specific patient.”
Putting Patients at Ease
Zara Patel, MD, assistant professor of otolaryngology-head and neck surgery and an expert in advanced endoscopic sinus and skull base surgery at Stanford University School of Medicine in Palo Alto, Calif., said that while patients want to know the risks of a procedure, it is incumbent on otolaryngologists to deliver the news in a way that avoids overly medical terms and minimizes anxiety. Of course, that conversation can be particularly difficult with rhinology procedures that involve operating in proximity to the brain and eyes.
“I go into specific risks regarding the area in which we’re working,” she said. “So, specifically for sinus surgery, I say, ‘You just want to remember that we’re working right around the eyes and right underneath the brain, and so, because we’re so close to those structures, I have to tell you that they are “at risk.” But, knowing the overall risk of those potential complications is less than 1% overall, you can feel comfortable that it’s really a minimal risk’ … Presenting it in that sort of fashion allows the patient to understand that [potential complications are] there, but they’re not some major thing that always happens that they have to focus on.”
Dr. Patel, who is also a co-author and editor of the textbook Office-Based Rhinology: Principles and Techniques (Plural Publishing Inc., 2013), said that while one reason for the process of informed consent is to protect the physician from liability, that is not the main purpose. Patients need this process to truly understand and weigh all the risks and benefits of their choice, and they can be frightened by jargon and confused by terms they’ve never heard.
Mostly, she said, patients just want to be comfortably prepared when facing a procedure. “Telling the patient how many of these procedures you have done can put them more at ease—and letting them know it is a very common procedure,” added Dr. Patel. “Often, when we do sinus surgery, we use
computer-guided navigation, and that can also make them feel a little bit more assured about it, even though there hasn’t been any evidence showing that its use decreases risk at all. … All those things kind of come into the conversation to allay their fears.”
Dr. Wolf said the best way to ensure that a patient’s consent is fully informed is to build a relationship. He noted the old adage that the best ways to avoid getting sued are “affability, availability, and ability—in that order.”
“It’s about building a rapport,” he added, acknowledging that this isn’t always easy to do, especially when physicians spend a lot of their time staring at computer screens when talking to patients, and when they need to see a certain number of patients within a certain period of time. However, he added, “If you have a relationship with your patient and they like you, they’re less likely to sue you,” he said.
Richard Quinn is a freelance medical writer based in New Jersey.
Key Points
- The process of informed consent protects the physician from liability and allows patients to understand all risks and benefits of their decision.
- Multimedia tools for patient education can be useful for otolaryngologists in clinical practice.
- A good way to ensure that a patient’s consent is truly informed is to build a relationship with that patient.
When a Patient Declines Consent
The process of obtaining informed consent is a double-edged sword for Leigh Sowerby, MD, and not because of litigation after obtaining said consent. “For me, the more frustrating thing is somebody who, after hearing the risks and benefits of surgery, decides that they don’t want surgery,” he said.
Take sinonasal surgery. “We’ll say there’s a risk we could injure your orbit and cause you to have decreased vision. And occasionally a patient will hear that and say, ‘Oh, I don’t want the surgery. There’s no way.’” He added, “To me, the most frustrating aspect of the informed consent process [is] when you know how much benefit a patient could potentially have from a procedure, but we have to respect their decision [to decline].”
Dr. Sowerby said that informed consent is more than getting patients to sign documentation allowing a procedure. It’s the process of making a patient understand why she’s signing. If a patient doesn’t sign, Dr. Sowerby sees it as his job to make his argument even stronger. “You just need to get to know that patient longer,” he added. “It means continuing on medical therapy, and seeing the patient back in three months, and seeing them back in another three months after that to develop a relationship, which then develops trust, which then ultimately allows the patient to let you help them.”