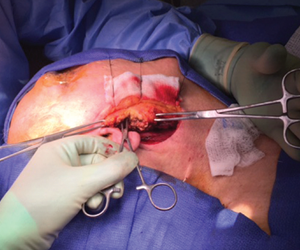
Parotidectomy.
© Nilesh Vasan, MD
SAN DIEGO—Head and neck surgery often involves finesse and preference, and techniques developed by a surgeon over time can be valuable to others if they’re shared. In that spirit, a panel of experts offered their insights and tips on a few common surgical procedures at the Annual Meeting of the American Academy of Otolaryngology-Head and Neck Surgery.
Explore This Issue
November 2016“There are tons of unmeasured variation, how we all do things differently,” said panel moderator Alexander Langerman, MD. “Wouldn’t it be cool if we could get a sense of how everybody’s doing everything so we have a bunch of tools in our box?”
The panel offered advice on glossectomy, tonsillectomy and neck dissection, and parotidectomy.
Glossectomy “Geppetto” Technique
Daniel Deschler, MD, vice chair of academic affairs for otolaryngology-head and neck surgery at the Massachusetts Eye and Ear Infirmary in Boston, presented the case of a 52-year-old man with a slow-growing lesion on the right lateral tongue that was 1.9 cm by 1.1 cm by 9 mm.
A biopsy found it was moderately differentiated squamous cell carcinoma. A computed tomography (CT) scan found there was no deep extension to the midline. There was no nodal involvement.
Dr. Deschler performed a partial glossectomy, with selective neck dissection, even though this was an N0 tumor, because the evidence shows there’s a benefit in doing so in these cases (N Engl J Med. 2015;373:521-529). For the Geppetto technique, named after the fictional woodcarver who crafted Pinocchio, Dr. Deschler offered these suggestions:
- Place sutures around the tongue lesion at 1 cm from the edge to get a 1 cm margin.
- Control the edges with the strings, like a puppeteer, as you do the mucosal incisions.
- Consider using a Colorado needle for the Bovie, and a harmonic scalpel. With these, he said, you get little to no bleeding and little char, making the sample easier for the pathologist to evaluate. “There’s not a lot of associated burn.”
- Aim for a specimen shaped “like a canoe”—deeper in the middle and more narrow and more shallow at the ends. This gives a well-defined specimen without taking extra tongue, he said.
- Mark the specimen with string. Dr. Deschler leaves a shorter string on the superior edge of the specimen—both “shorter” and “superior” start with “S”—so there’s no confusion once the specimen is at pathology.
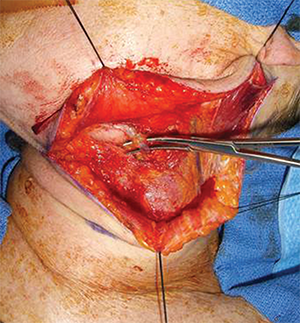
Division of the facial vein followed by superior retraction of the submandibular gland protects the marginal mandibular nerve without the need to identify it, while affording wide exposure to access level II of the neck.
© Courtesy Jeremy Richmon, MD