How does a novel, flexible, single-port robotic surgical system for transoral tongue base resection compare to the current multiport, rigid-arm robotic surgical system?
Bottom line
Surgical workflow was more streamlined with the da Vinci Sp system, and the new capabilities of simultaneous dissection, traction, and counter traction allowed for improved dissection and vessel control.
Explore This Issue
January 2018Background: Currently, transoral robotic surgery, designed for cardiac and abdomino-pelvic surgery, is the only commercially available robotic surgical system for multidisciplinary treatment for oropharyngeal squamous cell carcinoma. The da Vinci Si surgical robot’s dimensions are larger than what would be ideal for head and neck surgery, and it utilizes three rigid instrument arms that must approach transoral anatomy from a sometimes troublesome trajectory outside of the surgical field. The newer da Vinci Sp provides three fully articulating instruments delivered through a single 25-mm cannula entry port.
Study design: Preclinical anatomic study of four human cadavers using the da Vinci Si and the da Vinci Sp surgical robots.
Setting: Intuitive Surgical, Sunnyvale, Calif.
Synopsis: Successful completion of transoral resection of the tongue base was achieved in all four cadavers using both systems. Three cadavers were dentate and one was edentulous; no dental injury occurred in the three dentate cadavers, nor were there lip or facial abrasions. The default camera position (above) was utilized for the first Sp tongue base resection, but this configuration contributed to significant difficulty in visualization and dissection, resulting in a prolonged operative time of 23.25 minutes.
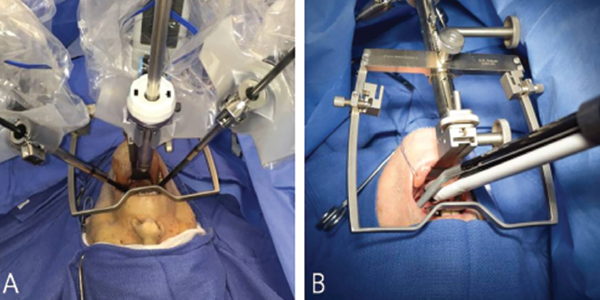
Comparison of bedside setup for robotic tongue base resection. Patient bedside setup of the flexible, single-port da Vinci Sp robotic surgical system (A) and the rigid, multiarm da Vinci Si robotic surgical system (B). The camera is positioned below in the da Vinci Sp’s cannula. The Sp system offers more space for the bedside surgical assistant.
© 2017 The American Laryngological, Rhinological and Otological Society, Inc.
For the next three Sp procedures, a more optimal configuration was utilized (operative time 6.22 to 8.85 minutes). For each procedure with the Si system, one instrument exchange occurred to facilitate better soft tissue handling as the specimen became larger and more difficult to grasp. Three-instrument operating with the Sp improved the ability to provide traction and counter traction on the soft tissues of the tongue base.
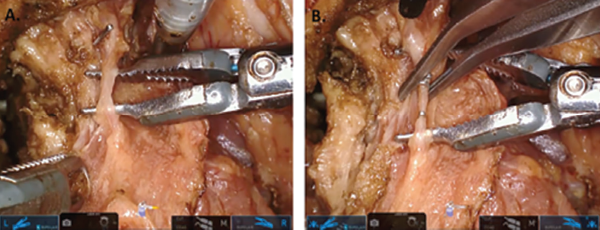
Isolation of small branching vessels with da Vinci Sp dual-forceps dissection. (A) The Maryland forceps (left) are providing traction and the fenestrated bipolar forceps (right) are being used to isolate a small branching vessel within the deep tongue musculature. The cautery spatula (top) is being used as a blunt retractor to provide slight counter traction. (B) The vessel has been isolated and is being controlled with surgical clips that are placed by the bedside assistant.
© 2017 The American Laryngological, Rhinological and Otological Society, Inc.