According to David M. Spiro, MD, MPH, associate professor of emergency medicine and pediatrics at Oregon Health and Science University in Portland, the lack of consistent use of pain medications, particularly in the Pittsburgh study, more than likely influenced the results. “It is likely there would be no statistically significant differences between the two groups if all patients in both groups had been given both oral analgesics and ear drops,” he said.
Explore This Issue
April 2011—Julie L. Wei, MD
Dr. Wei thinks the fact that all children in the study were not prescribed the routine use of pain medications may have introduced a flaw into the study. “When you’re looking at one intervention, you must control for all other factors,” she said, adding that treatment of pain in AOM can be highly effective and can influence whether or not antibiotics are prescribed.
Dr. Hoberman emphasized that no difference was found in the use of analgesics between the two groups and that the aim of the study was not to evaluate pain medication.
Dr. Lieberthal expressed doubts about the effect the use of analgesics would have on the primary outcomes of the studies.
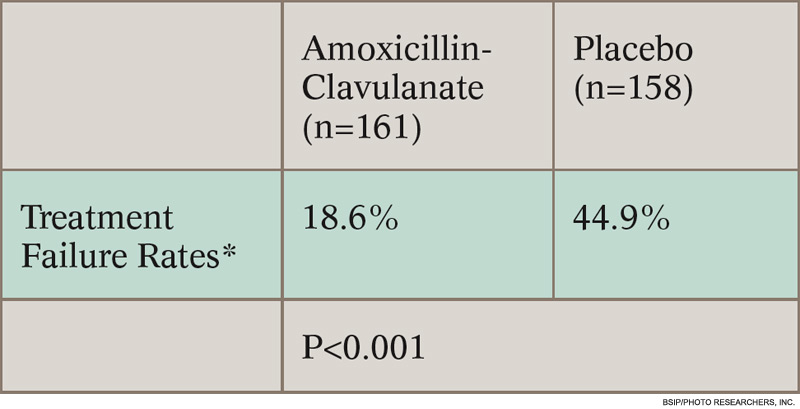
*Determined by composite of six components: no improvement in overall condition by day three, worsening of child’s overall condition, no improvement in otoscopic signs by day eight, perforation of the tympanic membrane, severe infection, any reason for stopping study drug.
Although it is uncertain whether the lack of consistent pain medication use introduced a variable that may have influenced the results of these studies, all experts consulted agree that better diagnosis of AOM may be the key to limiting antibiotic use.
Even with strict diagnostic criteria, however, whether or not to treat immediately may be a judgment call.
“I feel that the physician and parent, using shared decision making, may choose to observe initially and start antibiotics if symptoms persist,” Dr. Lieberthal said, reiterating that the majority of patients in the placebo groups of both studies improved despite meeting stringent diagnostic criteria.
Leave a Reply