


Presentation: A 33-year-old white male presented with a one-year history of right-sided odynophagia. Symptoms were constant and exacerbated by swallowing. He had a history of cryptic tonsils but had not undergone tonsillectomy; his past medical history was otherwise unremarkable. There was tenderness to palpation over the right tonsil with exacerbation of symptoms. No head and neck masses were appreciated. A CT scan was obtained (Figures 1, 2).
What’s your diagnosis? How would you manage this patient? Go to the next page for discussion of this case.
Management: The CT revealed bilateral elongated styloid processes, with the right styloid measuring 4 cm in length and terminating near the right palatine tonsil.
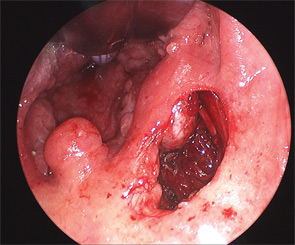
The patient was taken to the operating room, where a palatal incision was made superior to the tonsillar fossa, taking care to avoid injury to the tonsil (Figure 3). It has been the author’s experience that removal of the tonsil does not aid exposure and is not indicated in the absence of tonsillar pathology. Direct palpation of the styloid process is used to guide subsequent dissection, and the tensor palatini muscles overlying the styloid are bluntly elevated off the bone using a Freer elevator. A small rongeur is used to divide the distal 2 cm of the styloid process. At three weeks follow-up, the patient reported complete symptom resolution.
Discussion: Eagle’s syndrome describes a variety of head and neck pain symptoms that may occur secondary to an elongated styloid process. True Eagle’s syndrome is rare; the incidence of an elongated styloid process, defined as greater than 25 mm in length, ranges from 1.4 to 30 percent in the literature, but fewer than 10 percent of patients with an elongated styloid ever present with pain symptoms. Classic Eagle’s syndrome is described as pain from stimulation of cranial nerves IX and X and, at times, V and VII by an elongated styloid. Less commonly, it has been reported that an ossified stylohyoid or stylomandibular ligament may cause cervicalgia or odynophagia that is exacerbated by movement. Glossopharyngeal neuralgia is the most common manifestation of Eagle’s syndrome and the symptom most amenable to relief with a surgical approach when true Eagle’s syndrome is present.
A diagnosis of Eagle’s syndrome is a common referral in otolaryngology practice, but it is important to rule out other causes of pain before attributing symptoms to the styloid process. Because an elongated styloid is a common radiologic finding, confirmation of an association between the styloid process and symptoms may be sought by eliciting symptoms by transoral palpation of the styloid process, or by relieving pain using an injection of topical anesthetic into the tonsil fossa overlying the elongated styloid. If neither maneuver affects symptoms, then it is unlikely that Eagle’s syndrome is present, regardless of radiographic findings.
References
- Kim E, Hanson K, Frizzi. Eagle syndrome: case report and review of the literature. Ear Nose Throat J. 2008;87(11):631-633.
- Beder E, Ozgursoy OB, Ozgursoy SK. Current diagnosis and transoral surgical treatment of Eagle’s syndrome. J Oral Maxillifac Surg. 2005; 63(12):1742-1745.
—submitted by Christine G. Gourin, MD, FACS, associate professor of otolaryngology-head and neck surgery, Johns Hopkins University, Baltimore, Md.
Leave a Reply