Can anterior laryngeal electrodes (ALEs) help reduce the error of false positives in laryngeal nerve function assessment during thyroid and parathyroid surgery?
Bottom Line
Compared to ETT surface electrodes, ALEs provide similar and stable electromyographic responses with equal sensitivity during neural monitoring in thyroid and parathyroid surgery.
Explore This Issue
December 2018Background: Injury to the recurrent laryngeal nerve (RLN) with resultant vocal fold paralysis is one of the most significant complications of thyroid and parathyroid surgery. Intraoperative neural monitoring is a useful adjunct for the laryngeal nerve function assessment. Typically, electromyographic responses recorded by endotracheal tube (ETT) surface electrodes are monitored, but tube position alterations during surgery can cause displacement of the electrodes relative to the vocal cords, leading to false positive loss of signal.
Study design: Retrospective review of 15 consecutive patients undergoing thyroid and parathyroid surgery from April 27, 2016, to October 5, 2016, with intraoperative neuromonitoring using both ETT electrodes and ALEs.
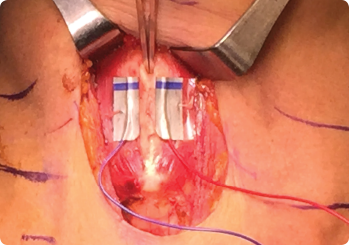
Anterior laryngeal electrode positioning on the laminae of the thyroid cartilage. Forceps indicate the midline thyroid cartilage notch.
© 2018 The American Laryngological, Rhinological and Otological Society, Inc.
Setting: Department of Otolaryngology–Head and Neck Surgery, Northwestern University Feinberg School of Medicine, Chicago.
Synopsis: With vagal stimulation, mean ipsilateral vocalis baseline electromyographic (EMG) amplitude was 924.44 ± 27.70 μV with ETT and 806.19 ± 131.43 μV with ALEs. Amplitudes were similar for right versus left vagus nerves, but mean latency for the left vagus was significantly longer than for the right for both ETT and ALEs. Contralateral vocalis mean amplitude and mean latency recorded by ETT during ipsilateral vagal stimulation were 156.81 ± 15.81 μV and 4.90 ms, respectively. With RLN stimulation, mean baseline EMG amplitude was 1341.88 ± 49.69 μV for ETT and 1117.64 ± 24.31 μV for ALEs. For both electrodes, mean EMG amplitudes and latencies were comparable for the right and left RLN, and mean amplitudes with RLN stimulation were significantly larger and latencies significantly shorter compared to vagal stimulation. The ALE EMG waveform with RLN stimulation showed robust biphasic morphology with the same polarity of deflection compared to the ETT ipsilateral vocalis waveform; both waveforms were better defined and more robust compared to the nontarget contralateral vocalis muscle. Upon external branch of the superior laryngeal nerve (EBSLN) stimulation, mean baseline EMG amplitude for right and left EBSLN combined was 286.89 ± 11.15 μV with ETT and 2315.63 ± 131.29 μV with ALEs.