INTRODUCTION
The nasal tip framework depends on the structural integrity of major and minor tip support mechanisms. The weakening of these supporting mechanisms is caused by the natural and physiologic process of aging, but it is also a common outcome of rhinoplasty surgery, particularly in those treated using an open approach. The common outcome for all patients with compromised structural integrity of nasal configuration is nasal tip ptosis, a common un-aesthetical facial deformity (Plast Reconstr Surg. 2012;129:118e–125e).
Explore This Issue
September 2023The columellar strut graft is among the techniques frequently used to enhance nasal tip aesthetics. It is employed to strengthen and lengthen the medial crura, correcting asymmetry, projection, and rotation of the nasal tip (Plast Reconstr Surg. 2012;129:118e–125e; Aesthet Surg J. 2020;40:NP65–NP71; Acta Otorhinolaryngol Ital. 2013;33:169–176; Arch Facial Plast Surg. 2005;7:176–184). The standard practice of inserting columellar struts would follow an open septorhinoplasty under direct identification of the medial crura; however, the constant search for minimally invasive techniques among facial plastic surgeons increasingly favors the use of endonasal approach techniques because they offer numerous advantages over the standard practice, such as reduced surgery time, concealed incisions, and quicker postoperative healing, while preserving nasal structural anatomy (Acta Otorhinolaryngol Ital. 2013;33:169–176).
Numerous techniques of endonasal graft placement and design have been described. The most widely used technique consists of inserting the columellar strut graft in the intercrural pocket through direct visualization via a columellar marginal incision. Another commonly described technique is the endonasal delivery technique, which delivers the lower lateral cartilage using a combination of marginal and intercartilaginous incisions (Acta Otorhinolaryngol Ital. 2013;33:169–176).
In this article, we provide a detailed description of our technique, consisting of the insertion of a standard columellar strut through a hemi-transfixion incision in an indirect retrograde fashion. We also describe its clinical relevance and its impact on patients after they have undergone routine septoplasty.
METHOD
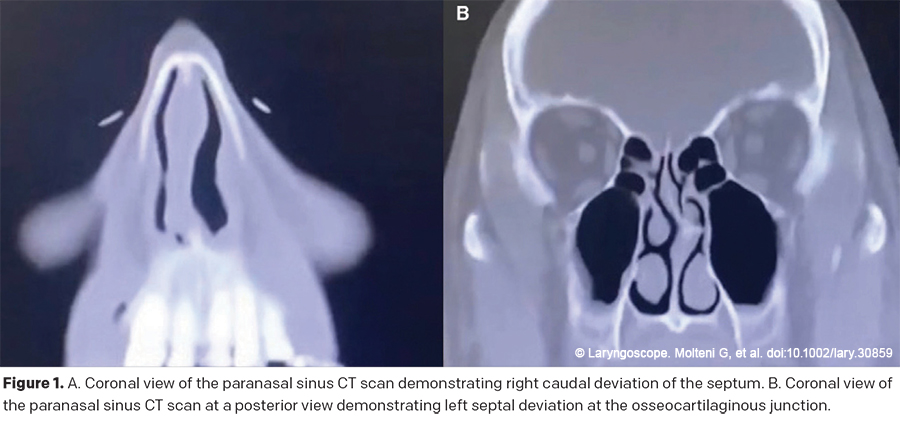
A 53-year-old male presented to our clinic with complaints of right nasal obstruction after a traumatic event to the face two years prior to his appointment. He denied additional sinonasal symptoms. Preoperative examination revealed no evidence of displaced nasal fracture and no palpable step-off. Facial evaluation showed adequate width and symmetry of the upper, middle, and lower nasal vault. Nasal tip evaluation showed a slightly bulbous tip with mild nasal flaring. Lateral examination revealed a mild dorsal hump and decreased nasolabial angle and projection. Basal view revealed caudal deviation of the columella toward the right. A paranasal sinus computerized tomography scan showed adequate nasal bone with healed comminuted fractures and an S-shaped deviation with a displacement of the anterior septum toward the right and posterior septum toward the left. After a conversation with the patient about the possible benefits and risks of surgery, he agreed to undergo a functional rhinoplasty, involving septoplasty with possible columellar strut graft.