 TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.com.
TRIO Best Practice articles are brief, structured reviews designed to provide the busy clinician with a handy outline and reference for day-to-day clinical decision making. The ENTtoday summaries below include the Background and Best Practice sections of the original article. To view the complete Laryngoscope articles free of charge, visit Laryngoscope.com.
Explore This Issue
June 2023BACKGROUND
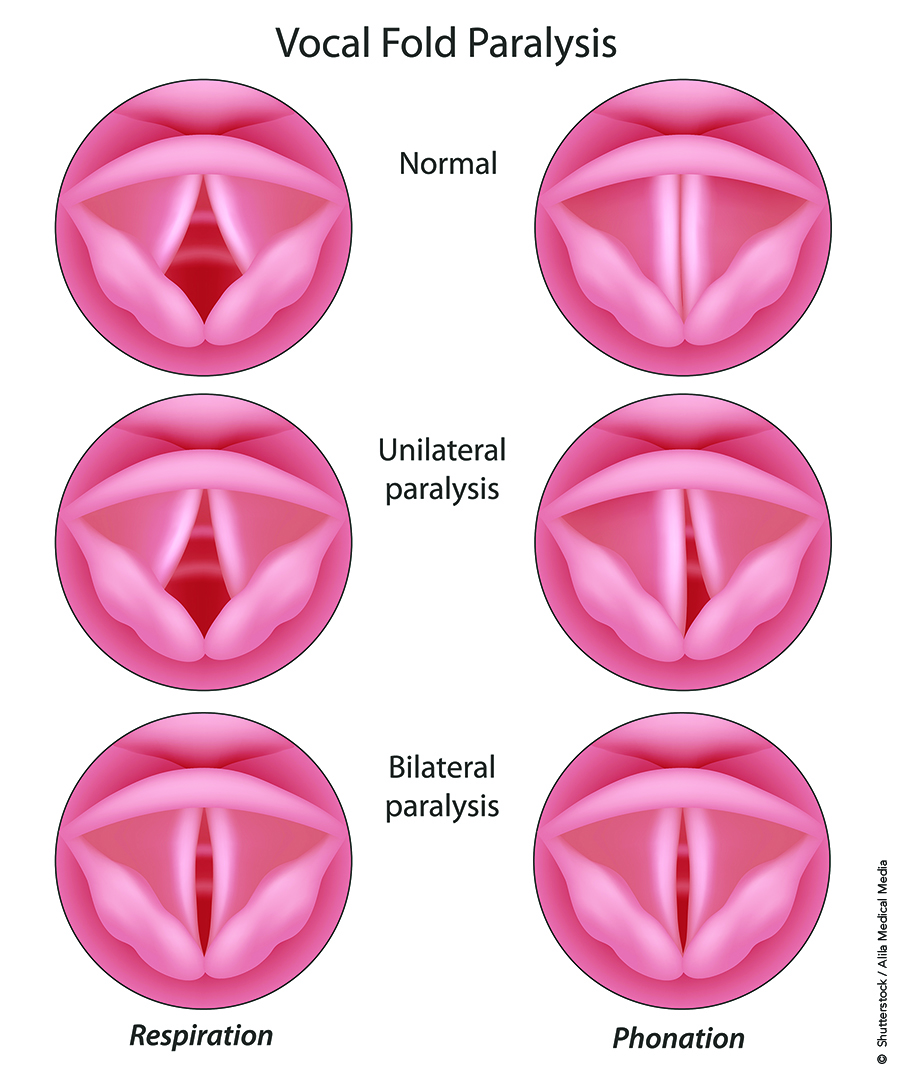
Unilateral vocal fold paralysis (UVFP) is a common condition presenting to the otolaryngologist. Injury to the vagal nerve or recurrent laryngeal nerve (RLN) results in a flaccid vocal fold and breathy dysphonia. Current management of UVFP includes injection augmentation, type 1 medialization thyroplasty, arytenoid adduction, laryngeal reinnervation (LR), or LR with a combination of static procedures.
The primary advantage of LR is prevention of denervation atrophy, which limits the long-term voice outcomes of static procedures. Recovery or maintenance of muscle tone from LR is expected to lead to more symmetric vibratory masses, symmetric mucosal wave propagation, and improved voice quality. The role of LR in management of adult UVFP remains controversial and is not fully established, however. Studies regarding the role of LR in UVFP vary considerably in design, quality, and level of evidence. Therefore, we evaluated the role of LR in the management of adults with UVFP. Within this review, we examined LR techniques, the role of laryngeal electromyography (LEMG) in decision-making for LR, the duration of denervation in decision-making for LR, whether age is a factor in decision-making, and the differences between LR and static procedures.
BEST PRACTICE
LR offers the possibility of restoring or maintaining muscle tone and bulk in the setting of UVFP and may provide the best quality voice in selected patients. Duration of denervation, preoperative innervation status, and age are considerations in choosing LR to treat UVFP. Patients who present within two years of injury and demonstrate denervation on LEMG have the best potential for voice improvement with LR. Additionally, younger patients demonstrate greater improvements following LR, although optimal cutoff age for LR candidacy remains to be established.
The most common LR procedure is ansa-RLN anastomosis, but direct nerve or neuromuscular pedicle implants are viable options. Adjunctive procedures, such as injection augmentation, medialization thyroplasty, or arytenoid adduction, may be considered at the time of LR to improve voice immediately in the postoperative period until voice improvement from reinnervation is established.
Standardization of outcome measures, clinical trials comparing static versus reinnervation procedures, and age-stratified studies can improve the quality of research in this area to further define the role of LR in the management of UVFP.